Cardiology PACS Systems, Features, CVIS Integration, and Workflow Benefits

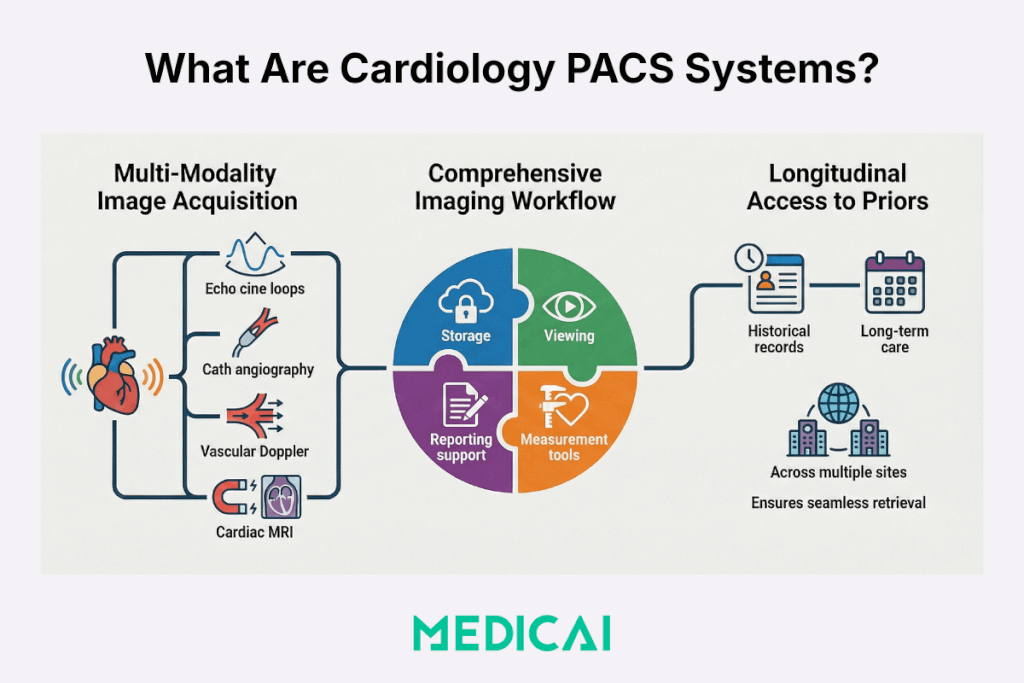
Cardiology PACS systems keep cardiovascular imaging usable, implied, not just stored. Cardiology PACS systems handle cine loops from echocardiography, angiography runs from catheterization, vascular ultrasound clips, and cardiac MRI series, and make priors easy to compare when the next follow-up arrives.
Cardiology teams feel the gap fast when playback stutters, measurements cannot be reused, or reports drift between systems. Cardiology PACS systems exist to address frictions in cine-first viewing, measurement capture, and structured reporting that persist after integration into CVIS and the EHR.

What are cardiology PACS systems, and what do they cover?
Cardiology PACS systems cover cardiovascular imaging workflows where cine loops, measurements, and procedure documentation define the reading and reporting requirements.
The systems start with image acquisition. Echocardiography produces cine loops and measurements that drive diagnosis and follow-up. Cardiac catheterization produces angiography runs and a procedure context that clinicians expect to find together. Vascular ultrasound produces Doppler-heavy studies that need smooth playback and consistent quantification. Cardiac MRI produces multi-series studies where priors comparison matters for longitudinal care.
The scope of Cardiology PACS systems includes the imaging record and the imaging workflow. It also contains storage, retrieval, viewing, measurement tools, reporting support, and sharing. The scope also comes with longitudinal access to prior records across sites, as cardiology care often spans years.
Which cardiology modalities and study types belong in cardiology PACS systems?
Cardiology PACS systems typically support the modality mix that cardiology teams read daily.
Study types that define cardiology PACS systems scope
- Echocardiography studies, transthoracic echo, stress echo, TEE, with cine loops and measurements
- Angiography studies, cath lab runs, and interventional imaging, with procedure context
- Vascular ultrasound studies, carotid, venous, and peripheral arterial exams, with Doppler and waveform review
- Cardiac MRI studies, multi-series cardiac imaging with functional and tissue characterization sequences
What does the cardiology PACS systems’ scope exclude, and where does CVIS start?
Cardiology PACS systems focus on imaging content and imaging workflow. CVIS, Cardiovascular Information System, focuses on the longitudinal cardiology record that connects imaging, procedures, hemodynamics, device data, scheduling, and documentation.
CVIS ownership usually includes procedure documentation and structured clinical data capture beyond images. CVIS ownership often includes cath lab documentation and hemodynamics capture. Cardiology PACS systems ownership usually includes the imaging archive, the cardiology viewer experience, and cardiology image distribution across teams.
What features do cardiology PACS systems need for echo and cath workflows?
Cardiology PACS systems feature a map to cardiology constraints, cine playback, measurements, structured reporting, and low-latency access to priors.
The system’s features are split into five capability groups.
- Cardiology viewing tools, cine controls, synchronized loop review, priors comparison
- Measurement tooling, echo quantification, ejection fraction workflows, reproducible calcs
- Structured reporting, device-to-report mapping, templates, and fewer manual fields
- Large study handling, streaming behavior, caching, server-side processing options
- Collaboration tooling, controlled sharing, review workflows, and audit visibility
Cardiology viewing tools
Cardiology viewing tools in the PACS systems prioritize cine playback and comparison. Cine review requires smooth frame stepping, play speed control, and consistent rendering across endpoints. Priors review requires fast side-by-side comparison, consistent layout behaviors, and predictable navigation across series.
Measurement tooling
Measurement tooling in cardiology PACS must reduce “measurement drift” between readers. Ejection fraction workflows often rely on consistent contouring and consistent calculation methods. Simpson’s Method supports echo teams because the platform requires stable tracing tools and reliable reporting fields tied to those measurements.
Structured reporting
Structured reporting in cardiology PACS systems reduces manual transcription. Structured reporting links measurements, findings, and procedure context into templated outputs. Cath lab workflows benefit when key procedure values map into report fields without retyping.
Large study handling
Large study handling in cardiology PACS systems targets responsiveness under load. Cardiology studies can include many cine loops, many series, and high data volume. Server-side rendering and streaming architectures help when endpoints vary, remote reading exists, or IT teams want fewer workstation installs.
Collaboration tooling
Collaboration tools in PACS systems support multidisciplinary decision-making. Cardiology care often involves imaging review by cardiologists, radiologists, surgeons, and referring physicians. Controlled sharing requires access controls, audit logging, and secure distribution paths.
What structured reporting capability closes the biggest workflow gap?
Cardiology PACS systems close the largest workflow gap by capturing measurements once and reusing them throughout the report lifecycle.
Structured reporting features that matter most
- Auto-populated fields from measurements and modality metadata
- Report states that match operations, draft, preliminary, final, and addendum
- Template governance that keeps service-line reporting consistent across sites
- Export patterns that keep the report usable inside the EHR
What data handling requirements show up in real cardiology datasets?
Cardiology PACS encounter data patterns that differ from those in routine radiology.
Cardiology data handling requirements that drive platform design
- Many instances per study due to cine loops and multiple views
- Mixed content types, still frames plus moving video, waveforms when present
- High demand for priors because cardiology follow-up depends on longitudinal comparisons
- Time sensitivity in urgent workflows such as cath lab escalations and acute echo reads
How do cardiology PACS systems integrate with CVIS and EHR?
Cardiology PACS systems integration succeeds when patient identity, accession context, and report delivery stay consistent across CVIS and the EHR.
The PACS systems rarely operate alone. Cardiology PACS systems live inside a workflow that starts with scheduling and ends with a signed report in the EHR. CVIS integration matters because CVIS often owns the cardiology procedure context and structured clinical data. EHR integration matters because clinicians expect imaging access inside the patient chart.
Which standards typically power cardiology PACS systems integration?
Cardiology PACS systems integration usually relies on three interoperability standards.
Integration standards that show up most
- DICOM, Digital Imaging and Communications in Medicine, for imaging objects, storage, and transport
- HL7 v2, Health Level Seven, for demographics, orders, and results messaging in many hospitals
- FHIR, Fast Healthcare Interoperability Resources, for modern API-based integration patterns in app ecosystems
DICOM ties the images and metadata to a standards-based imaging object. HL7 ties the imaging workflow to enterprise scheduling and results delivery. FHIR ties the imaging experience to modern applications and patient-context launches.
What does “unified patient record” mean in cardiology PACS systems terms?
A unified patient record means the EHR becomes a launch point for imaging studies with correct context, correct identity, and consistent access controls.
Unified record behaviors that clinicians notice
- One-click access from the EHR chart to the cardiology PACS systems viewer
- Correct grouping of studies by patient and encounter, not by manual workarounds
- Report availability next to images, with a status that matches clinical reality
- Priors visibility across sites, so longitudinal cardiology care stays continuous
Which integration failures break cardiology PACS systems workflows?
Cardiology PACS systems failures cluster into predictable patterns that impact patient safety, throughput, and trust.
Integration failures that break cardiology PACS workflows
- Patient ID mismatch, wrong chart linkage, and wrong priors
- Accession mismatch, orphan studies that never reconcile to an order
- Missing order context, worklist drift, and manual entry spikes
- Report delivery failure, report stuck outside the EHR, and downstream delays
- Latency and timeouts, cine playback degradation during peak reading hours
Patient identity failures create the worst clinical risk. Accession failures create the worst operational friction. Latency failures create the fastest clinician backlash because cine review becomes painful.
What strategic benefits do cardiology PACS systems deliver to cardiology operations?
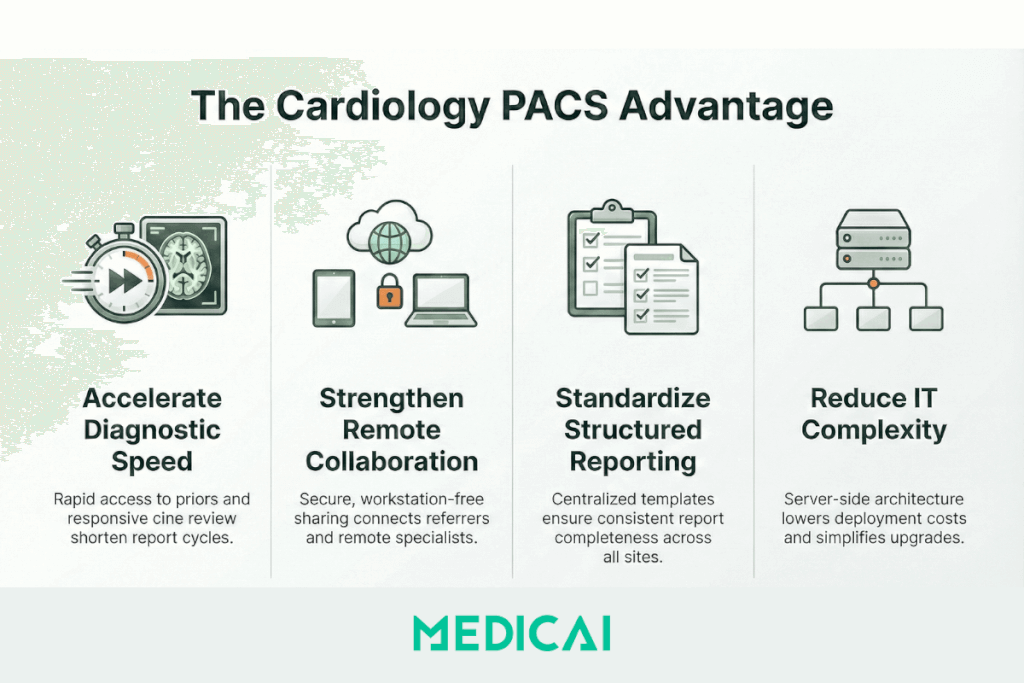
Cardiology PACS systems’ benefits show up as faster access to priors, tighter collaboration, and lower operational friction across multi-site cardiology services.
The benefits of cardiology PACS systems fall into four measurable outcomes.
- Diagnostic speed, fewer steps to priors, faster cine review, shorter report cycles
- Collaboration, secure sharing with referrers, and remote specialists
- Standardization, consistent structured reporting across cardiologists and sites
- Cost and IT load, fewer endpoint installs in web patterns, simpler upgrades, clearer lifecycle planning
Diagnostic speed
Cardiology PACS systems improve diagnostic speed when priors retrieval becomes predictable, and cine review stays responsive. Cardiology PACS systems reduce friction when measurements and report fields are tightly linked. Cardiology PACS systems help when clinicians avoid hunting for studies across multiple archives.
Collaboration
Cardiology PACS systems strengthen collaboration when sharing stays are controlled and fast. Remote review workflows matter for outreach clinics and multi-site networks. Referring physicians value access that does not require special workstations.
Standardization
Cardiology PACS systems support standardization through templates and shared measurement practices. Structured reporting reduces variation in report completeness. Governance becomes easier when templates live centrally, and updates propagate consistently.
Cost and IT load
Cardiology PACS systems reduce IT load when deployment complexity drops. Thin-client and server-side architectures reduce dependence on workstations. Centralized updates reduce version drift across endpoints. Lifecycle planning improves when data retention and migration plans are in place before the archive fills.
Buying clarity, standalone specialty system vs enterprise platform
Cardiology PACS system buying decisions depend on where your complexity lies: within cardiology only or across the enterprise.
Decision cues that separate the two paths when you are struggling to find the most suitable PACS vendors for cardiology.
- A standalone cardiology PACS system fits private practices and single-service-line groups that need fast echo and vascular workflows without an enterprise imaging scope.
- An enterprise imaging approach suits hospitals and IDNs that need a single longitudinal imaging record across radiology, cardiology, and other departments.
Medicai supports cardiology PACS systems workflows when teams want web access, multi-site collaboration, and clean integration into broader imaging operations. We help most when cardiology imaging needs to travel across sites without losing identity, context, or priors continuity.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo