Benefits and Challenges of Interoperability in Healthcare: A Complete Guide

Healthcare interoperability is the ability of different clinical systems, devices, and applications to exchange and use patient data effectively across organizational boundaries. The benefits are substantial: better-coordinated patient care, reduced duplicate testing, faster diagnoses, improved population health management, and lower operational costs across the healthcare system. The challenges are equally substantial: technical incompatibility between legacy systems, inconsistent data standards, security and privacy risks, high implementation costs, regulatory complexity, and organizational resistance to change.
Healthcare leaders evaluating interoperability investments need to understand both sides clearly, because the decisions about which standards to adopt, which systems to integrate, and which workflows to redesign depend on weighing concrete benefits against concrete barriers.
This guide covers the seven primary benefits of healthcare interoperability, the seven primary challenges of interoperability in healthcare, the standards and frameworks (HL7, FHIR, USCDI, TEFCA) that make interoperability technically possible, and the practical approaches healthcare organizations use to overcome the most common implementation barriers.
| Dimension | Benefits | Challenges |
|---|---|---|
| Patient care | Complete patient view across providers, fewer medical errors, faster diagnoses, better-coordinated treatment | Identity reconciliation across systems, split records, incomplete data despite connection |
| Operations | Reduced duplicate testing, automated workflows, less manual data entry, faster billing cycles | Workflow disruption during implementation, ongoing interface maintenance burden |
| Standards and technology | HL7 FHIR APIs, DICOMweb, USCDI data exchange, TEFCA national framework | Technical incompatibility, inconsistent standards implementation, legacy system integration |
| Cost | Lower long-term operational costs, reduced duplicate imaging and testing, improved revenue cycle | High initial investment, ongoing licensing and maintenance, specialized integration staff |
| Security and privacy | Standardized authentication, encryption-by-default, comprehensive audit trails | Expanded attack surface, HIPAA compliance complexity, cross-organizational consent management |
| Population health | Disease tracking, public health reporting, clinical research at scale, quality measure reporting | Data quality variability, missing data elements across sources, governance for shared data sets |
| Patient experience | Patient portal access, transferable records, third-party app integration, patient-controlled sharing | Inconsistent portal capabilities across providers, identity verification across organizations |
What is healthcare interoperability, and why does it matter
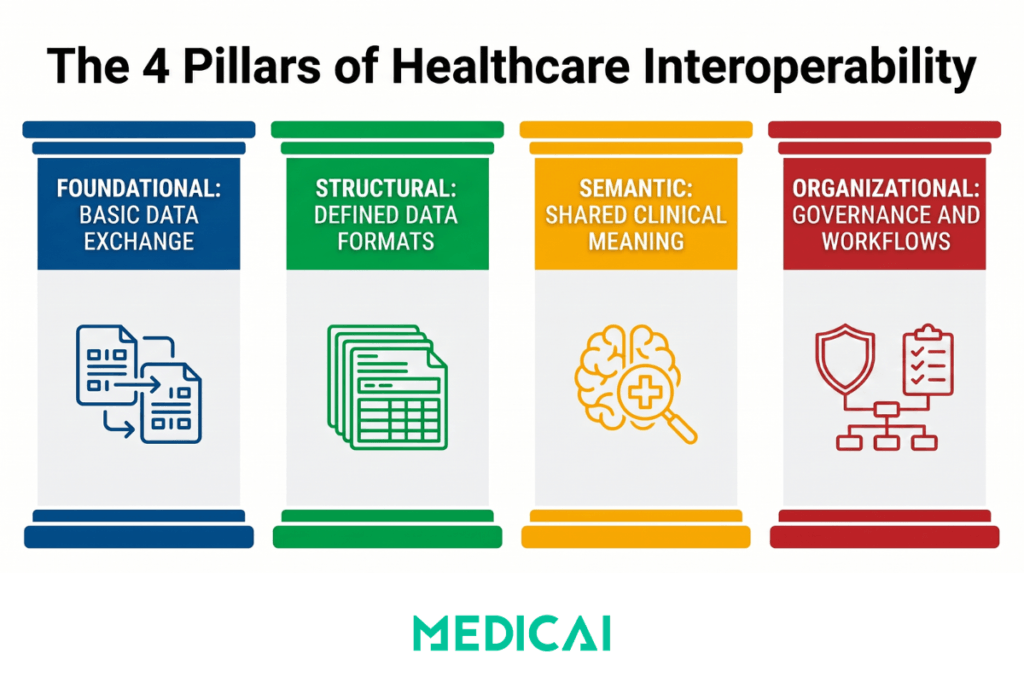
Healthcare interoperability is the capacity of different clinical systems, medical devices, and software applications to exchange patient data, access shared information, and use that information cooperatively across organizational boundaries. The Healthcare Information and Management Systems Society (HIMSS) defines four levels of interoperability that healthcare leaders should understand.
Foundational interoperability is the ability to exchange data between two systems, with no specific structure required for the receiving system to interpret it. Structural interoperability provides a defined data format and structure, enabling receiving systems to parse incoming messages reliably. Semantic interoperability adds shared meaning, so the receiving system not only parses the data but also understands what each element represents clinically. Organizational interoperability encompasses the governance, policies, and workflows that enable data to flow effectively across organizational boundaries, with appropriate consent and use controls.
Most discussions of healthcare interoperability focus on the structural and semantic levels, where standards such as HL7 V2, FHIR, DICOM, LOINC, SNOMED CT, and ICD-10 define data formats and clinical meaning. But organizational interoperability is often where real-world implementations succeed or fail, because the technical capability to exchange data does not guarantee that organizations will agree on how to use it.
The reason healthcare interoperability matters now is that patient care increasingly happens across multiple providers, settings, and time periods. A patient’s primary care, specialty care, hospital encounters, imaging studies, lab results, prescriptions, and patient-reported data all need to flow into a coherent clinical record. Without interoperability, that record stays fragmented across many separate systems, and clinicians make decisions with incomplete information. With interoperability, the patient’s clinical context follows them, improving care quality.
For deeper technical coverage of how interoperability standards work, see the What Is HL7 guide.
The benefits of interoperability in healthcare
Healthcare interoperability delivers measurable benefits across seven dimensions. Each benefit has a direct clinical, operational, or financial impact that healthcare organizations can quantify when evaluating interoperability investments.
1. Better-coordinated patient care
Interoperability gives clinicians a comprehensive view of patient health across all care settings. A primary care physician sees specialty consultations. A specialist sees prior imaging and labs from the patient’s other providers. An emergency department clinician sees the patient’s medication list, allergies, and recent hospitalizations. Clinical decision-making improves because decisions are based on complete information rather than on what the patient remembers or what arrived via fax.
Care transitions specifically benefit from interoperability. Hospital discharge to skilled nursing facility, specialty referral, transition from pediatric to adult care, transfer between health systems — each transition is a moment where missing information causes care quality to degrade. Interoperability minimizes the information loss at these transitions.
2. Reduced medical errors and improved patient safety
Most medical errors trace back to missing or incorrect information at the point of decision. A clinician prescribing a medication without knowing the patient’s list of allergies. A radiologist interpreting an imaging study without access to prior comparisons. A surgeon planning a procedure without a complete history of prior surgeries or implants. Interoperability addresses these information gaps directly, with measurable reductions in medication errors, duplicate imaging, and adverse drug events in healthcare systems that have implemented robust interoperability.
3. Lower operational costs and reduced duplicate testing
Duplicate imaging studies and laboratory tests account for substantial waste in US healthcare. Patients who change providers, receive care across multiple health systems, or move between primary and specialty care often have tests repeated because prior results are inaccessible. Interoperability reduces this waste by making prior results available at the point of care. The cost savings benefit both healthcare organizations (by reducing unnecessary testing costs) and patients (by reducing copays, contrast exposure from repeat CTs, and inconvenience).
4. Streamlined clinical workflows and reduced administrative burden
Interoperability automates workflows that previously required manual data entry, faxing, or phone calls. Lab orders flow automatically from the EHR to the laboratory information system. Imaging results are returned to the ordering provider via HL7 messaging or FHIR APIs. Referrals carry the complete patient context to the receiving specialist. Each automated workflow reduces administrative burden on clinical staff and shortens the time from order to result.
5. Improved population health management and clinical research
Interoperability enables population-scale analyses that single-organization data cannot support. Public health surveillance for disease outbreaks, clinical quality measure reporting, comparative effectiveness research, and value-based care quality measurement all require data aggregated across multiple organizations. Health Information Exchanges (HIEs), TEFCA-participating Qualified Health Information Networks (QHINs), and clinical research networks all depend on interoperability infrastructure.
6. Better patient engagement and self-management
Patient portals, personal health record applications, and third-party health apps require API-based access to clinical data. Interoperability through FHIR APIs is what makes patient-facing applications possible. Patients with access to their complete clinical record become more engaged in their care, manage chronic conditions more effectively, and catch potential issues earlier than patients with fragmented access to their records.
7. Innovation enablement for AI and clinical decision support
Modern AI clinical decision support tools, predictive analytics, and ambient documentation systems depend on access to comprehensive clinical data. The applications that promise to transform healthcare delivery, AI-augmented diagnosis, automated risk stratification, and clinical workflow optimization all require interoperability as a foundation. Healthcare organizations with strong interoperability infrastructure can adopt new clinical AI tools faster than organizations whose data stays trapped in disconnected silos.
For organizations integrating medical imaging into the broader clinical data exchange, medical imaging EHR integration patterns cover the specific approaches that work in radiology workflows.
The challenges of interoperability in healthcare
The benefits above are real, but achieving them in practice faces seven recurring obstacles that healthcare organizations consistently encounter during interoperability implementations. Understanding these challenges helps healthcare leaders plan realistic timelines and budgets, rather than discovering the obstacles mid-project.
1. Technical incompatibility between systems
Different healthcare organizations use different EHR systems, medical devices, laboratory information systems, and clinical software. Even when systems claim to support the same standards (HL7 V2, FHIR, DICOM), the specific implementation choices vary in ways that prevent clean integration. One EHR uses different segment ordering in HL7 messages than another. One PACS uses non-standard DICOM tag implementations. One laboratory information system populates fields differently than the receiving EHR expects. These small incompatibilities add up to substantial integration work for every new connection.
2. Inconsistent data standardization
Healthcare data uses multiple competing coding systems and terminologies. Diagnoses can be coded in ICD-10, SNOMED CT, or local codes. Lab results can use LOINC codes or proprietary identifiers. Medications can be referenced by RxNorm, NDC, or vendor codes. Procedures can use CPT, HCPCS, or ICD-10 PCS. Mapping between these terminologies during data exchange introduces errors and ambiguity. The 21st Century Cures Act and USCDI requirements have improved standardization for the most critical data elements, but substantial variation remains across the broader clinical data set.
3. Data security and privacy risks
Interoperability inherently expands the attack surface for healthcare data. More systems exchanging data means more endpoints to secure, more authentication and authorization decisions to manage, and more opportunities for breaches. HIPAA compliance complexity grows with the number of business associates handling PHI. Cross-organizational data sharing requires a consent management infrastructure that many healthcare organizations have not built. Ransomware attacks on healthcare systems have increased dramatically, with interoperability connections sometimes serving as the entry vector for broader network compromises.
4. Legacy systems that were not designed for interoperability
Many healthcare organizations still operate clinical systems from the 1990s and 2000s, designed before modern interoperability standards existed. These legacy systems may have limited HL7 V2 capabilities and no FHIR support, rely on proprietary data formats, or run on operating systems that no longer receive security updates. Upgrading or replacing legacy systems is expensive, disruptive, and operationally risky, but maintaining them limits the interoperability the organization can achieve.
5. High costs of implementation and ongoing maintenance
Interoperability implementation requires investment in integration software (interface engines, integration platforms), specialized integration engineering staff, ongoing maintenance of the connections as systems evolve, security monitoring, and regular audits. The initial implementation cost for a hospital system implementing modern interoperability infrastructure can reach millions of dollars. Ongoing operational costs include licensing for interface engines, integration platform fees, and staff to monitor and maintain the connections. Smaller practices often cannot afford the full interoperability stack.
6. Organizational resistance to change
Healthcare organizations resist change for predictable reasons. Existing workflows have organizational momentum that new interoperable workflows must overcome. Clinical staff have become accustomed to the current systems and resist retraining. IT departments protect the systems they understand. Vendors sometimes resist interoperability because it threatens vendor lock-in. Leadership may be skeptical that interoperability investments deliver returns within practical time horizons. The result is that even when the technical capability exists, the organizational change required to use it effectively often fails to occur.
7. Regulatory and governance complexity
Healthcare interoperability operates within a complex regulatory environment. HIPAA governs privacy and security. The 21st Century Cures Act mandates the prevention of information blocking. ONC certification establishes EHR requirements. State laws add jurisdiction-specific requirements. Cross-border data flows trigger international regulations. Organizations must navigate this complexity while implementing technical interoperability, a process that requires legal and compliance expertise, which many healthcare organizations lack in-house. Governance frameworks for cross-organizational data sharing add another layer of complexity that takes time to establish.
Standards and frameworks that enable interoperability
Healthcare interoperability is built on specific technical standards and regulatory frameworks. Healthcare leaders evaluating interoperability investments should understand which standards their organizations need to support.
HL7 V2 remains the dominant messaging standard for real-time clinical workflows, including orders, results, and admission, discharge, and transfer events. Most hospital interoperability still runs on V2 messaging via interface engines. See What Is HL7 for the detailed coverage of V2 and its message types.
HL7 FHIR is the modern API-based standard mandated by the 21st Century Cures Act for certified EHR API access. FHIR adoption has accelerated dramatically since 2020, driven by regulatory pressure, patient empowerment use cases, and modern cloud architectures. New healthcare integrations are increasingly FHIR-first. See HL7 FHIR vs HL7 V2 for the architectural comparison.
DICOM handles medical imaging data exchange, with DICOMweb providing modern API-based imaging access alongside FHIR for clinical data. See What Is DICOM is for imaging-specific interoperability standards.
USCDI defines the minimum data set that certified EHRs must support for interoperability, updated annually by the ONC. Healthcare organizations need to verify that their EHR systems support current USCDI versions.
TEFCA establishes the national framework for health information exchange through Qualified Health Information Networks (QHINs). TEFCA participation enables cross-organizational data exchange at a national scale.
HIPAA, the 21st Century Cures Act, and state regulations provide the legal framework within which all healthcare interoperability operates. The compliance requirements affect implementation choices and ongoing operational responsibilities.
For organizations focused on functional interoperability specifically — the capability for systems to exchange data effectively in clinical workflows — see Functional Interoperability in Healthcare for that focused coverage.
How healthcare organizations overcome interoperability challenges
The challenges above are real but not insurmountable. Healthcare organizations that have successfully implemented interoperability share recognizable patterns in their approach to the work.
Start with clear use cases and prioritize accordingly. Organizations that attempt to interconnect everything at once typically fail. Organizations that identify specific high-value use cases (closing the loop on imaging results to referring physicians, automating laboratory order entry, enabling care coordination across affiliated practices) and implement them sequentially deliver value while building organizational capability.
Invest in interface engine infrastructure or modern integration platforms. Healthcare interoperability at scale requires middleware that handles message routing, transformation, monitoring, and error recovery. Interface engines (Rhapsody, Corepoint, Mirth Connect, others) are the traditional choice. Cloud-based integration platforms increasingly handle the same workload with the convenience of managed services. The choice depends on organizational scale, existing infrastructure, and available technical staff.
Establish governance for cross-organizational data sharing. Technical capability without organizational agreement does not produce interoperability. Healthcare organizations need governance frameworks specifying which data flows where, with what consent, under what use restrictions, and with what audit and monitoring. Established governance frameworks, such as the TEFCA Common Agreement, provide templates for organizations joining national health information networks.
Plan for ongoing operational investment, not just one-time implementation. Interoperability is not a project with an end date. It is an ongoing operational capability that requires monitoring, maintenance, staff skill development, and regular updates as standards evolve. Organizations that treat interoperability as project-based work struggle when the project ends and the connections begin to degrade. Organizations that treat it as an ongoing operational capability sustain the benefits.
Choose vendors with strong interoperability commitments. Healthcare technology vendor selection significantly affects long-term interoperability. Vendors that openly publish their FHIR API capabilities, participate in industry interoperability initiatives, and avoid information-blocking practices are better long-term partners than vendors that treat interoperability as an afterthought.
For a modern cloud-native imaging architecture that supports HL7 messaging, FHIR APIs, and DICOMweb, see Medicai’s cloud PACS platform and imaging-EHR integration patterns.
Frequently asked questions about healthcare interoperability
Healthcare interoperability is the ability of different clinical systems, medical devices, and software applications to exchange and use patient data across organizational boundaries. HIMSS defines four levels: foundational (basic data exchange), structural (defined format), semantic (shared meaning), and organizational (governance and workflows). Modern healthcare interoperability is built on standards including HL7 V2, HL7 FHIR, DICOM, USCDI, and the TEFCA national framework.
The main benefits of healthcare interoperability include better-coordinated patient care across providers, reduced medical errors through comprehensive patient data access, lower operational costs through reduced duplicate testing, streamlined clinical workflows that reduce administrative burden, improved population health management and clinical research, better patient engagement through portal access, and innovation enablement for AI and clinical decision support tools. Each benefit translates to measurable improvements in care quality and operational efficiency.
The seven primary challenges to healthcare interoperability are technical incompatibility between systems, inconsistent data standardization across coding systems, security and privacy risks from expanded attack surface, legacy systems not designed for modern interoperability, high implementation and maintenance costs, organizational resistance to workflow change, and regulatory complexity spanning HIPAA, the Cures Act, ONC certification, and state laws. Each challenge requires deliberate planning to overcome.
Interoperability is important because patient care increasingly happens across multiple providers, settings, and time periods, and clinical decisions improve when clinicians have complete patient information rather than fragmented records. Interoperability reduces medical errors, eliminates duplicate testing, supports care coordination across providers, enables population health management, and provides the data foundation for AI clinical decision support tools. The Cures Act and TEFCA make interoperability increasingly mandatory rather than optional.
The main standards supporting healthcare interoperability include HL7 V2 for real-time clinical messaging, HL7 FHIR for modern API-based exchange, DICOM for medical imaging, LOINC for laboratory observations, SNOMED CT for clinical terminology, ICD-10 for diagnoses, RxNorm for medications, and CPT for procedures. The 21st Century Cures Act mandates FHIR APIs for certified EHRs. USCDI defines the required minimum data set. TEFCA establishes the national framework for cross-organizational data exchange.
HIPAA establishes the privacy and security requirements that all healthcare interoperability must comply with. The Privacy Rule governs how patient data can be shared and requires patient consent for specific use cases. The Security Rule requires encryption, access controls, audit logs, and other technical safeguards. The Breach Notification Rule requires reporting of data breaches. Interoperability does not bypass HIPAA, it operates within HIPAA. The compliance complexity grows with the number of participating organizations and connections.
Costs vary significantly by organization size and scope. Initial implementation for a hospital system can reach millions of dollars covering integration software, infrastructure, specialized staff, and process redesign. Ongoing maintenance includes interface engine licensing, integration platform fees, integration engineering staff, security monitoring, and regular audits. Smaller practices typically operate at lower scale through EHR-provided integration capabilities and cloud-based platforms. Cost-benefit analysis should factor reduced duplicate testing, faster billing cycles, and improved revenue cycle management against implementation cost.
TEFCA (Trusted Exchange Framework and Common Agreement) is the national framework for health information exchange in the United States, established by the 21st Century Cures Act and operationalized by ONC starting in 2022. TEFCA defines how Qualified Health Information Networks (QHINs) connect to enable nationwide healthcare data exchange. TEFCA’s technical foundation is FHIR-based with USCDI data elements. Healthcare organizations participating in TEFCA gain access to nationwide data exchange that previously required individual bilateral agreements.
The path forward for healthcare interoperability
Healthcare interoperability is moving from optional to mandatory through regulatory pressure, from regional to national through TEFCA, and from messaging-based to API-based through FHIR adoption. Healthcare organizations that treat interoperability as a strategic capability rather than a compliance burden are positioned to deliver better care, operate more efficiently, and adopt new clinical technologies faster than organizations that resist the transition.
The benefits described in this guide are real and measurable when interoperability is implemented thoughtfully. The challenges are also real but follow predictable patterns that experienced healthcare IT teams can plan for. The organizations succeeding with interoperability share recognizable characteristics: clear use case prioritization, investment in modern infrastructure, governance frameworks for cross-organizational data sharing, ongoing operational commitment rather than project-based thinking, and vendor selection that prioritizes long-term interoperability.
For healthcare organizations starting their interoperability journey or expanding existing capabilities, the practical next steps include auditing current data exchange capabilities against USCDI requirements, evaluating FHIR API support across current vendor systems, planning TEFCA participation if cross-organizational exchange is strategically important, and investing in the operational capability (staff, monitoring, governance) that sustainable interoperability requires.
For deeper coverage of the standards underlying healthcare interoperability, see What Is HL7. For the comparison between modern and legacy HL7 standards, see HL7 FHIR vs HL7 V2. For functional interoperability specifically, see Functional Interoperability in Healthcare. For imaging-specific interoperability, see What Is DICOM and Medical Imaging EHR Integrations.

Related Articles

Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo