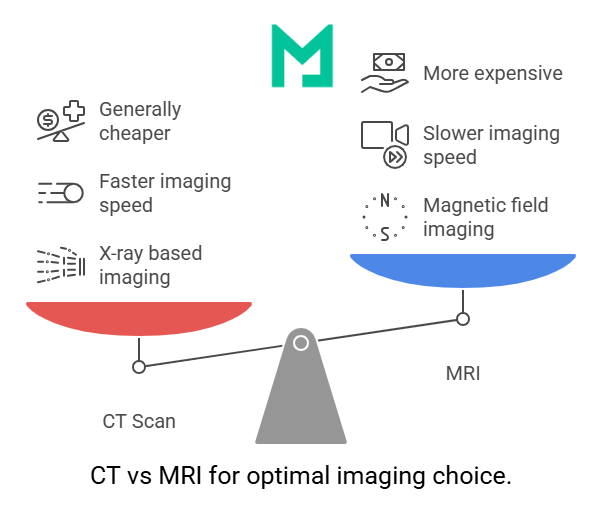
MRI vs CT Scan: Differences, Uses, Cost, and How Doctors Choose Between Them

The main difference between MRI vs CT scan is the technology: MRI (magnetic resonance imaging) uses powerful magnets and radio waves to produce detailed images of soft tissues without radiation, while CT (computed tomography) uses X-rays to produce rapid cross-sectional images, particularly well-suited for bone, lung, and acute trauma evaluation. MRI typically takes 30-60 minutes and excels at imaging the brain, spinal cord, muscles, ligaments, and organs. CT typically takes 5-15 minutes and excels at emergency situations, fractures, and rapid assessment. The choice between them depends on what the doctor needs to see, how quickly results are needed, and patient-specific factors like pregnancy, claustrophobia, or implants.

How MRI and CT scans work
MRI and CT scans use fundamentally different technologies to produce medical images. Understanding how each works clarifies why they’re suited to different clinical situations.
MRI (magnetic resonance imaging) uses a powerful magnetic field (typically 1.5 Tesla or 3 Tesla) and radio waves to produce images of the body. The patient lies inside a tube-shaped scanner that generates the magnetic field. When the magnet activates, hydrogen atoms inside the body’s water and fat align with the field. Radio waves are then pulsed at specific frequencies, causing the hydrogen atoms to release energy signals that the scanner detects. A computer reconstructs these signals into highly detailed cross-sectional images. The process involves no radiation. MRI scans typically take 30-60 minutes, depending on the body part and protocol.
CT (computed tomography) uses X-rays in a different geometry than traditional radiography. An X-ray tube rotates around the patient inside a donut-shaped scanner, sending X-ray beams through the body from many angles. Detectors on the opposite side measure how much radiation passes through, and a computer reconstructs the data into cross-sectional images. The process exposes the patient to ionizing radiation, though diagnostic CT doses are typically within safe ranges under established protocols. CT scans typically take 5-15 minutes.
The technology difference drives the clinical difference. MRI’s magnetic field interacts with the body’s hydrogen content, which makes it exceptional for soft tissue contrast (different tissues have different water content). CT’s X-rays interact with tissue density, making it exceptional for showing bone, calcifications, hemorrhage, and density-based contrast.
Both technologies have evolved significantly since they became clinical standards. Modern MRI machines (3T and emerging 7T systems) produce dramatically more detailed images than the early scanners of the 1980s. Modern CT scanners use lower radiation doses than older systems while producing better images, and dual-energy CT and photon-counting CT are pushing capabilities further. The basic technology comparison remains: MRI for soft tissue, CT for speed and bone, with both continuing to improve.
Key differences between MRI and CT scans
The differences between MRI and CT scans go beyond technology to include scan time, radiation exposure, image quality for different tissues, cost, accessibility, and contraindications. Understanding these differences across multiple dimensions helps clarify why doctors choose one over the other for specific clinical situations. The comparison below covers the practical differences patients and clinicians most often need to know.
| Dimension | MRI | CT Scan |
|---|---|---|
| Technology | Magnetic field and radio waves, no ionizing radiation | X-rays from multiple angles, uses ionizing radiation |
| Scan time | 30 to 60 minutes typically, depending on body part and protocol | 5 to 15 minutes typically, including positioning and processing |
| Best for soft tissue | Excellent detail for brain, spinal cord, muscles, ligaments, tendons, and internal organs | Good general detail, less differentiation between similar soft tissues |
| Best for bone | Limited bone detail, but excellent for bone marrow and surrounding soft tissue | Exceptional bone detail, the imaging standard for fractures and bony pathology |
| Emergency suitability | Too slow for most acute emergencies, limited availability outside business hours | Fast enough for emergency use, widely available 24/7 in hospital settings |
| Radiation | None, making MRI preferable for pediatric, pregnant, or frequent imaging needs | Uses ionizing radiation, with cumulative exposure considered in repeat imaging decisions |
| Contrast | Gadolinium-based contrast for vascular, tumor, and inflammation evaluation | Iodine-based contrast for vascular studies, tumor characterization, and bowel evaluation |
| Typical cost | $400 to $3,000 without insurance, depending on body part and facility type | $300 to $1,500 without insurance, generally lower than equivalent MRI |
| Contraindications | Pacemakers, some implants, severe claustrophobia, certain metal foreign bodies | Pregnancy (when avoidable), iodine contrast allergy, severe kidney disease for contrast studies |
| Patient experience | Loud, enclosed (closed MRI) or open architecture, requires lying still 30 to 60 minutes | Quieter, more open scanner, requires lying still only 5 to 15 minutes |
When doctors choose MRI vs when they choose CT
The clinical decision between MRI and CT depends on what the doctor needs to see and how quickly. Several patterns guide which scan gets ordered.
Doctors typically choose MRI when the clinical question involves soft tissue detail, slow-evolving conditions, or situations where radiation exposure should be avoided. Brain tumors and multiple sclerosis appear far more clearly on MRI than CT. Ligament tears, cartilage damage, and muscle injuries that CT shows poorly are clearly visible on MRI. Spinal cord pathology requires MRI to see the cord itself, even when CT can show the surrounding bone. For pediatric patients, pregnant patients, and patients who need repeat imaging over months or years, MRI’s lack of radiation often makes it the preferred choice when both technologies could answer the clinical question.
Doctors typically choose CT when the clinical situation is acute, when speed matters more than soft tissue detail, or when bone or lung evaluation is central to the diagnosis. Trauma patients arriving at emergency departments routinely receive a CT scan because it provides results in minutes, when time matters. Suspected acute hemorrhage (in the brain or abdomen) appears clearly on CT, often more reliably than on MRI for fresh bleeding. Bone fractures, particularly subtle ones, are CT’s domain. Lung pathology, kidney stones, and most acute abdominal complaints get CT as the first imaging step because of its speed and broad diagnostic utility.
For some clinical questions, the choice is genuinely close, and the doctor’s preference, scan availability, and patient factors determine the order. Stroke evaluation often uses CT first to rule out hemorrhage, then MRI to evaluate the brain in detail. Some cancer staging protocols use both — CT for the chest and abdomen, and MRI for the brain or specific organs.
Cost and accessibility also factor into the decision. CT is generally cheaper, faster, and more widely available than MRI. For clinical questions where both could work, CT often wins on practical grounds even when MRI would give marginally better images.
The clinical decision is always physician-led, not patient-chosen. Patients sometimes assume one technology is “better” and request it, but the right choice depends on the specific clinical question, the patient’s history, and the practical realities of imaging availability in the local healthcare system.
MRI vs CT scan cost and accessibility
Cost is one of the most practical differences between MRI and CT scans, and it influences both physicians’ ordering patterns and patients’ out-of-pocket costs.
Without insurance, an MRI typically costs $400 to $3,000, depending on the body part, whether contrast is used, and where the scan is performed. Hospital MRI sits at the higher end of this range; dedicated imaging centers and urgent care MRI typically run in the middle; and basic non-contrast MRI at the lowest-cost facilities sits at the bottom of the range.
CT scans typically cost $300 to $1,500 without insurance, generally cheaper than an equivalent MRI for the same body part. The cost difference reflects shorter scan time, lower equipment costs, and broader availability — CT machines are more common than MRI machines across US healthcare facilities.
With insurance, out-of-pocket costs depend on the specific plan, deductible status, and whether the imaging facility is in-network. Most insurance plans cover medically necessary imaging, whether MRI or CT, but pre-authorization is often required for both. High-deductible plans can result in high out-of-pocket costs for either scan.
Accessibility differs meaningfully. CT scanners are available in essentially every hospital and most urgent care facilities. MRI machines are more limited — many smaller hospitals have only one MRI scanner, urgent care MRI is still uncommon, and scheduling an MRI can take days or weeks at busy facilities. For emergency situations or time-sensitive clinical questions, accessibility often pushes the decision toward CT even when MRI would provide marginally better images.
For patients comparing options, the practical cost order (lowest to highest) is typically: dedicated imaging center, urgent care, hospital. The same order applies to both MRI and CT. Pre-authorization protects against denied claims, regardless of facility choice.
MRI vs CT scan safety considerations
Safety considerations differ significantly between MRI and CT because the two modalities pose distinct risks.
CT scans use ionizing radiation. A single chest CT exposes the patient to roughly 7 millisieverts (mSv) of radiation, equivalent to about 2-3 years of natural background radiation exposure. The doses for diagnostic CT are considered acceptable for clinical benefit, but cumulative radiation exposure is a concern for patients receiving frequent CT scans. For pediatric patients (more radiation-sensitive than adults) and pregnant patients (for whom fetal radiation exposure is avoided when possible), the radiation risk often favors MRI or ultrasound when those alternatives can answer the clinical question.
MRI uses no ionizing radiation, eliminating that specific concern. The safety considerations for MRI are different. The strong magnetic field is dangerous to anyone with pacemakers, certain implanted medical devices, cochlear implants, or metal foreign bodies that could move or heat up in the field. Pre-MRI safety screening identifies these contraindications. Modern pacemakers and many implants are MRI-conditional (safe under specific conditions), but the screening still happens for every patient.
Gadolinium contrast (used in some MRIs) is generally well tolerated but is avoided in patients with severe kidney disease due to the rare risk of nephrogenic systemic fibrosis. Iodine contrast (used in some CTs) is also generally well-tolerated but carries a small risk of allergic reaction and is used cautiously in patients with kidney disease.
Claustrophobia affects MRI more than CT. Unline open MRI, closed MRI scanners have a long, narrow tunnel that some patients find difficult to tolerate during 30-60-minute scans. Options include open MRI machines, sedation, or alternative imaging when claustrophobia is severe.
For most patients undergoing either scan, the safety profile is well-established, and the clinical benefit clearly justifies the procedure.
Which is better for specific conditions: MRI or CT scan
The “which is better” question depends entirely on the specific clinical condition. The patterns below cover the most common imaging questions.
For brain imaging, CT is preferred for acute symptoms (stroke screening, head trauma, suspected hemorrhage) because it produces fast results that can guide immediate treatment decisions. MRI is preferred for non-acute brain evaluation — tumors, multiple sclerosis, dementia workup, subtle stroke evaluation, and detailed brain anatomy. For a more detailed comparison covering the clinical decision framework, see MRI vs CT for brain.
For spine imaging, CT shows bony anatomy (fractures, spinal stenosis from bone, spondylolysis) better than MRI. MRI shows the spinal cord, nerve roots, intervertebral discs, and surrounding soft tissue better than CT. Many spine evaluations use CT first for bone and MRI second for soft tissue, or skip directly to MRI when the clinical question is disc disease, nerve compression, or spinal cord pathology.
For abdominal imaging, CT is the first imaging step for most acute abdominal complaints — appendicitis, kidney stones, bowel obstruction, and abdominal trauma. CT is fast, evaluates both bone and soft tissue, and works well even when the differential diagnosis is broad. MRI of the abdomen is used for specific clinical questions — liver lesions, pancreatic evaluation, biliary tree imaging — where MRI’s superior soft-tissue contrast adds diagnostic value.
For chest imaging, CT dominates because lung tissue does not image well on MRI. Pulmonary nodules, pneumonia, pulmonary embolism, lung cancer staging, and chest trauma all use CT. MRI of the chest is reserved for specific clinical questions, such as cardiac imaging or evaluation of mediastinal masses, where MRI with contrast helps.
For musculoskeletal imaging, MRI is the imaging of choice for ligament injuries, cartilage damage, muscle injuries, and tendon tears. CT is preferred for complex fractures, especially fractures involving multiple bone fragments, where 3D reconstruction guides surgical planning. Sports medicine imaging leans heavily on MRI for soft-tissue evaluation.
For trauma evaluation, CT is the first imaging step in most emergency departments because it can rapidly evaluate the head, chest, abdomen, and pelvis in a single comprehensive workup. MRI is performed during the recovery phase if specific clinical questions remain after the initial CT.
For pediatric imaging, the radiation risk often favors MRI or ultrasound when those alternatives can answer the clinical question, with CT reserved for situations where speed matters more than radiation avoidance.
How to know which scan you need
The choice between MRI and CT is a clinical decision made by the ordering physician based on the specific diagnostic question. Patients don’t typically choose directly between MRI and CT, but understanding the decision framework helps facilitate informed conversations.
Three questions guide the physician’s decision. First, what is the clinical question — is the doctor looking for soft tissue detail, bone detail, acute pathology, or something else? Second, how quickly are results needed — is this an emergency, or can the patient wait for a scheduled scan? Third, are there patient-specific factors — pregnancy, pacemaker, claustrophobia, kidney disease, contrast allergies — that affect the choice?
The doctor weighs these factors against the available imaging at the specific facility. A small hospital with only a CT scanner and limited MRI access may use CT for clinical questions that a larger facility would address with an MRI. A large academic medical center may have more options and order more MRIs for the same clinical scenarios.
When patients want to ask informed questions, helpful queries include: what the doctor is specifically looking for, why this scan over the alternative, what does the scan involve from the patient’s perspective (preparation, time, contrast, anything to avoid), and what happens after the scan based on different possible findings.
For specific scenarios — comparing MRI with other modalities, choosing among MRI machine types, or evaluating MRI across different facility types — the MRI Comparisons guide covers the full set of MRI decisions in one place.
Frequently asked questions about MRI vs CT scan
The main difference between MRI and CT scan is the technology: MRI uses magnetic fields and radio waves with no radiation, while CT uses X-rays with ionizing radiation. MRI excels at soft tissue detail (brain, spinal cord, muscles, ligaments, organs) and takes 30-60 minutes. CT excels at bone, lung, and acute trauma evaluation and takes 5-15 minutes. The clinical choice depends on what the doctor needs to see and how quickly.
Neither MRI nor CT is universally better — each excels at different clinical situations. MRI is better for soft tissue detail, brain tumors, spinal cord evaluation, and ligament injuries, and uses no radiation. CT is better for bone fractures, lung pathology, acute hemorrhage detection, and emergency situations where speed matters. For most clinical questions, one is clearly preferred based on what the doctor needs to evaluate.
MRI is typically more expensive than CT scan for the same body part. Without insurance, MRI costs $400-$3,000 while CT costs $300-$1,500. The cost difference reflects MRI’s longer scan time, higher equipment costs, and the specialized technicians required. Insurance typically covers both when medically necessary, but pre-authorization requirements often apply. Out-of-pocket costs depend on the specific plan and deductible status.
MRI uses no ionizing radiation, making it safer in that specific regard, particularly for pediatric patients, pregnant patients, and patients requiring repeat imaging. CT uses ionizing radiation at doses considered acceptable for clinical benefit but accumulating with repeat imaging. However, MRI’s strong magnetic field is dangerous for patients with pacemakers, certain implants, or metal foreign bodies. Both are safe for most patients when appropriate screening is done.
CT is significantly faster than MRI. A CT scan typically takes 5-15 minutes including positioning and processing. An MRI typically takes 30-60 minutes depending on the body part and protocol. The speed difference is why CT is preferred for emergency situations where minutes matter, and MRI is used for non-acute imaging where detailed soft tissue evaluation matters more than scan time.
The choice depends on the clinical situation. CT is preferred for acute brain symptoms — suspected stroke (to rule out hemorrhage), head trauma, sudden severe headache — because it produces fast results for time-sensitive treatment decisions. MRI is preferred for non-acute brain evaluation — tumors, multiple sclerosis, subtle strokes, dementia workup, detailed brain anatomy — because it shows soft tissue detail CT cannot match.
MRI and CT show different aspects of the body, and each can show some things the other cannot. MRI shows soft tissue, brain, spinal cord, ligaments, and organ detail that CT cannot match. CT shows bone, lung tissue, and acute hemorrhage clearly, with some scenarios where CT outperforms MRI. For many clinical questions, both can show the relevant pathology, but with different levels of detail and different acquisition patterns. The choice depends on what the doctor specifically needs to evaluate.
CT uses ionizing radiation; MRI does not. A typical chest CT exposes the patient to about 7 millisieverts of radiation, equivalent to 2-3 years of natural background radiation. The doses are considered acceptable for diagnostic benefit, but cumulative exposure matters for patients receiving frequent CT scans. MRI uses magnetic fields and radio waves with no radiation exposure, making it preferable when the clinical question allows either technology and radiation exposure is a concern.
The choice between MRI and CT scan is a clinical decision made by the doctor based on what they need to evaluate, how quickly results are needed, and patient-specific factors like pregnancy, implants, or kidney function. Patients don’t typically choose between the two, but understanding the framework helps with informed conversations. Ask the doctor what they’re looking for, why this scan over the alternative, and what the scan involves from the patient’s perspective.
Both MRI and CT typically produce results within 24-48 hours after the scan, though urgent or emergency scans may be read within hours. CT scans are sometimes read by an emergency radiologist immediately when ordered in the emergency department, particularly for trauma or acute symptoms. MRI scans typically take slightly longer to read because the studies contain more detailed images that require careful evaluation. Specific timing depends on the facility’s radiology workflow.

Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo