MRI Comparisons: Different Types of MRI, Machines, Procedures, and Imaging Alternatives

Different types of MRI scans, machines, and procedures fit different clinical situations. Choosing the right MRI option, or deciding whether an MRI is the right scan at all, depends on what the doctor is looking for, the part of the body being imaged, the patient’s medical history, and practical considerations like comfort and availability.
This MRI comparisons guide compares the most common MRI options across four dimensions: MRI versus other imaging modalities (CT, MRA, EEG), MRI machine variations (open versus closed, 1.5T versus 3T), MRI procedure variations (with versus without contrast, hospital versus urgent care), and MRI for specific clinical questions. Each comparison links to a dedicated guide with the full clinical details.
Why patients and clinicians compare MRI options
MRI is one of the most versatile imaging tools in medicine, which means patients and clinicians often face choices about which type of MRI is best suited to a specific situation. The choices break down into four practical decision categories, each driven by a different clinical or logistical question.
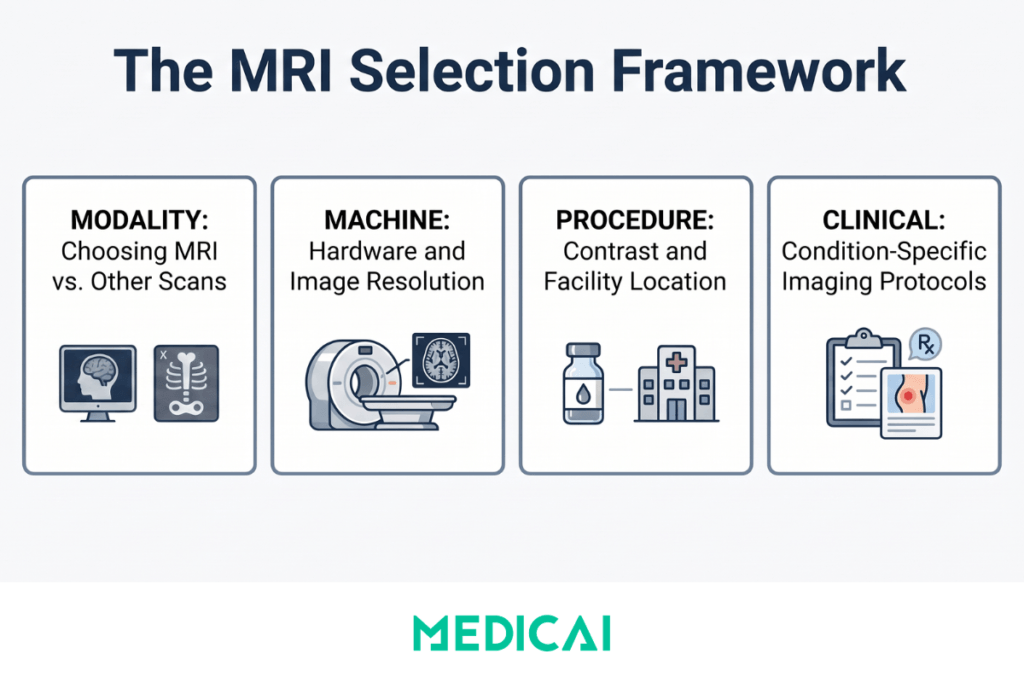
The first category is modality choice, whether MRI is the right scan at all, or whether a CT, MRA, ultrasound, or other imaging study would answer the clinical question more efficiently. MRI excels at soft tissue detail (brain, spinal cord, muscles, ligaments, internal organs) but takes longer than CT and isn’t suitable for emergency situations where speed matters more than detail. Choosing between MRI and another modality usually comes down to what the doctor needs to see.
The second category is machine choice, whether to use an open MRI, a closed MRI, a 1.5 Tesla machine, or a 3 Tesla machine. Open versus closed imaging affects patient comfort (open machines reduce claustrophobia) but comes at the expense of some image quality. 1.5T versus 3T affects image resolution and scan time, with 3T producing more detailed images but requiring careful protocol matching to the clinical question.
The third category is procedure choice: whether the MRI is performed with or without contrast, and where the scan is performed (a hospital radiology department, an outpatient imaging center, or an urgent care location). Contrast (gadolinium) is added when the doctor needs to evaluate blood vessels, tumors, inflammation, or scar tissue, but is avoided when not clinically necessary because of cost, time, and rare safety considerations. Location affects availability, cost, and the range of clinical questions the imaging can answer.
The fourth category is clinical-specific choice, comparing imaging options for a particular condition or symptom. MRI of the brain for symptoms might be compared with CT for the same indication. MRI for prostate evaluation has specific protocols tied to PSA levels. MRI for joint pain may be compared with ultrasound, depending on the structure being evaluated.
The sections below organize the major MRI comparisons by these four decision categories. Each comparison links to a dedicated guide with the full clinical details.
MRI compared to other imaging modalities
The most common MRI comparisons question is whether MRI is the right scan or whether another imaging modality would work better for the specific clinical situation. Three comparisons cover the majority of these decisions.
MRI vs CT scan. MRI uses powerful magnets and radio waves to image soft tissues in detail. CT uses X-rays to produce cross-sectional images quickly. MRI excels at brain tumors, spinal cord injuries, ligament tears, and detailed soft-tissue evaluation. CT excels at acute trauma, bone fractures, lung disease, and emergency situations where speed matters. The choice often comes down to whether the clinical question is “what’s the soft tissue detail” (MRI) or “what’s the immediate emergency picture” (CT). For the full comparison covering scan time, radiation exposure, contrast use, cost, and specific clinical scenarios, see MRI vs CT Scan: What Is The Difference.
MRI vs MRA. MRA (Magnetic Resonance Angiography) is a specialized MRI technique focused on imaging blood vessels rather than general anatomy. Standard MRI produces detailed images of organs, tissues, and structures; MRA produces detailed images of arteries and veins. The two studies use the same MRI machine but apply different acquisition protocols. MRA is the imaging modality of choice for suspected vascular disease (aneurysms, stenosis, vascular malformations), while standard MRI addresses a broader range of soft-tissue diagnostic questions. For deeper coverage of the protocols, indications, and how the two studies differ in practice, see Difference Between MRI and MRA.
MRI vs EEG. This comparison most often arises in neurology, where both studies are sometimes ordered for similar symptoms (seizures, headaches, neurological changes). MRI images the brain’s structure: tumors, strokes, multiple sclerosis lesions, and anatomical abnormalities. EEG measures the brain’s electrical activity in real time: seizure detection, epilepsy diagnosis, and sleep disorders. The two studies answer fundamentally different questions and are often complementary rather than alternative. For the full breakdown of what each study can and cannot show, see What Can an EEG Show That an MRI Cannot.
MRI vs CT for brain imaging specifically. When the clinical question is a brain symptom (headache, suspected stroke, possible tumor), the MRI vs CT decision becomes more nuanced. CT is faster and better for acute hemorrhage (the “is the brain bleeding right now” question). MRI is better for tumors, multiple sclerosis, subtle strokes, and detailed brain anatomy. The choice depends on whether the situation is acute or evaluative. See Which Is Better: MRI or CT Scan for Brain? for the clinical decision framework.
Different types of MRI machines
Beyond the modality question, patients facing an MRI often encounter choices about which type of MRI machine to use. Two comparisons dominate this decision.
Open MRI vs closed MRI
Closed MRI machines are the traditional design: a tunnel-shaped scanner that the patient slides into for imaging. Open MRI machines have a more open architecture with less enclosure, designed primarily to reduce claustrophobia for patients who find closed scanners distressing. The tradeoff is image quality: closed MRI machines typically have stronger magnetic fields and produce higher-resolution images than open MRI machines. For most diagnostic questions, closed MRI is the clinical preference; open MRI is appropriate when patient anxiety or physical constraints make closed MRI impractical. The full comparison covering image quality, scan time, claustrophobia management, weight limits, and clinical suitability is at Open MRI vs Closed MRI.
1.5 Tesla vs 3 Tesla MRI
Tesla (T) measures the strength of an MRI machine’s magnetic field. 1.5T and 3T are the two clinical standards, with 3T being twice as powerful as 1.5T. The stronger field produces higher-resolution images and shorter scan times, but requires careful protocol selection because some clinical scenarios actually image better at 1.5T (certain pediatric cases, patients with specific implants, claustrophobia-sensitive patients in older 3T designs). For routine imaging, both fields work well; for high-detail neurological, musculoskeletal, and cardiac imaging, 3T offers meaningful advantages. The detailed comparison is at 1.5T vs 3T MRI.
MRI procedure variations
Beyond machine choice, MRI procedures vary in ways that affect what the scan can show and where it can happen.
MRI with versus without contrast
Contrast agents (gadolinium-based for MRI) enhance the visibility of blood vessels, tumors, inflammation, and scar tissue by changing how those tissues appear on the scan. MRI without contrast is used for general anatomical evaluation, structural assessment, and routine screening. MRI with contrast is used when the doctor specifically needs to evaluate tumor characteristics, infection, inflammation, vascular abnormalities, or post-surgical changes. The decision is clinical: contrast is added when the diagnostic question requires it and avoided when not clinically necessary, since contrast adds time, cost, and rare safety considerations. The full guide on when each protocol applies is at MRI With Contrast.
MRI at urgent care vs hospital
Some urgent care facilities now offer MRI capabilities for situations where a patient needs imaging quickly but doesn’t require full emergency department services. MRI at urgent care is appropriate for acute orthopedic injuries (suspected ligament tears, fractures that need soft-tissue evaluation), some neurological symptoms (sudden severe headache without other emergency signs), and follow-up imaging for known conditions. Hospital MRI remains appropriate for complex cases, multi-modality workups, or situations where the clinical picture is unclear. The detailed guide on what urgent care MRI can and cannot do is at MRI at Urgent Care.
MRI for specific clinical questions
Some MRI comparisons aren’t about MRI versus another modality or one type of MRI versus another. They’re about whether MRI is the right next step for a specific clinical question.
MRI for prostate evaluation after PSA elevation. When PSA (prostate-specific antigen) levels rise above certain thresholds, prostate MRI is often the recommended next imaging step. The MRI evaluates the prostate for suspicious lesions that might warrant biopsy. The exact PSA threshold for ordering an MRI depends on age, prior PSA history, family history, and other risk factors. For the framework that guides this decision, see What is a Dangerous PSA Level MRI.
MRI for brain symptoms. As covered above, the choice between MRI and CT for brain symptoms depends on whether the clinical picture is acute (CT favored for speed and hemorrhage detection) or evaluative (MRI favored for tumors, MS, and detailed anatomy). The decision framework is at Which Is Better: MRI or CT Scan for Brain?.
For specific clinical scenarios not covered by a dedicated guide, the general decision principles apply: MRI excels at soft-tissue detail and slow-evolving conditions; CT excels at acute situations and bone evaluation; and the right choice depends on what the doctor needs to see and how quickly.
High-level MRI comparison cheat sheet
The table below summarizes the major MRI decision points at a glance. Each row links to the dedicated guide with full clinical detail. This cheat sheet is useful for patients preparing for an MRI conversation with their doctor or for clinicians orienting a new team member to the MRI decision landscape.
| Decision Category | Comparison | Choose This For |
|---|---|---|
| Modality choice | MRI vs CT scan | MRI for soft tissue detail and slow-evolving conditions, CT for acute trauma, bone, and emergency imaging |
| Modality choice | MRI vs MRA | MRI for general anatomy and soft tissue, MRA for blood vessels and vascular disease |
| Modality choice | MRI vs EEG | MRI for brain structure and anatomy, EEG for brain electrical activity and seizures |
| Machine type | Open vs closed MRI | Closed for image quality and routine diagnostic work, open for claustrophobia or physical constraints |
| Machine type | 1.5T vs 3T MRI | 1.5T for routine imaging and most clinical questions, 3T for high-detail neurological, musculoskeletal, and cardiac imaging |
| Procedure variation | With vs without contrast | With contrast for tumors, infection, inflammation, vascular abnormalities, post-surgical evaluation; without contrast for general anatomy and routine screening |
| Location | Urgent care vs hospital MRI | Urgent care for acute orthopedic injuries and clear single-question imaging, hospital for complex cases and multi-modality workups |
| Clinical-specific | MRI vs CT for brain | CT for acute brain symptoms and suspected hemorrhage, MRI for tumors, MS, subtle strokes, and detailed brain anatomy |
| Clinical-specific | Prostate MRI for elevated PSA | When PSA levels rise above clinical thresholds and additional evaluation is warranted before biopsy |
The cheat sheet shows that most MRI decisions are not about whether MRI is the right scan, but about which type of MRI fits the specific clinical question. The dedicated guides linked above cover each comparison in clinical detail. For questions not covered by a specific guide, the general principle holds: MRI excels at soft tissue and slow-evolving conditions, with the specific protocol, machine, and procedure determined by what the clinician needs to see.
Frequently asked questions about MRI comparisons
Different types of MRI scans include standard MRI (general anatomy and soft tissue imaging), MRA (magnetic resonance angiography for blood vessels), functional MRI (fMRI, for brain activity), diffusion-weighted MRI (DWI, for stroke and tumor evaluation), MR spectroscopy (chemical composition of tissues), and breast MRI (specialized breast imaging). MRI machines also vary by magnetic field strength (1.5T, 3T, 7T) and design (open vs closed). The right type depends on what the doctor needs to evaluate.
The MRI type is decided by the ordering physician based on the clinical question. Patients don’t typically choose between MRI types directly, but understanding the options helps with informed conversations. Key decision factors include what part of the body is being imaged, whether the focus is anatomy or function, whether blood vessels need evaluation (MRA), whether contrast is clinically necessary, and patient-specific factors like claustrophobia (open vs closed) or implants (which affect 3T suitability).
MRI uses powerful magnets and radio waves to image soft tissues in detail without radiation. CT uses X-rays for fast cross-sectional imaging, better for bone and acute trauma. Ultrasound uses sound waves, useful for some soft tissues and pregnancy. PET uses radioactive tracers to image metabolic activity. Each modality answers different clinical questions, and the choice depends on what the doctor needs to see, how quickly, and any safety considerations specific to the patient.
Neither is universally better, each excels at different clinical situations. MRI is better for soft tissue detail (brain tumors, spinal cord, ligaments, organs), uses no radiation, and shows subtle changes that CT can miss. CT is faster (seconds vs minutes), better for acute trauma and emergency situations, superior for bone fractures and lung disease, and more widely available. For brain symptoms specifically, CT is preferred for acute hemorrhage and MRI for everything else.
Closed MRI machines have a tunnel-shaped scanner that produces higher-resolution images with stronger magnetic fields (typically 1.5T or 3T). Open MRI machines have a more open architecture designed to reduce claustrophobia, but typically use weaker magnetic fields (often 0.3T to 0.7T) which can affect image quality for some clinical questions. Closed MRI is the clinical default; open MRI is appropriate when patient anxiety, body size, or physical constraints make closed scanning impractical.
The decision is clinical, not patient-chosen. Contrast (gadolinium for MRI) is added when the doctor needs to evaluate tumors, infections, inflammation, vascular abnormalities, or post-surgical changes, situations where contrast highlights specific tissue characteristics. MRI without contrast is sufficient for general anatomical evaluation, screening, and many routine diagnostic questions. The ordering physician decides based on the clinical question, with consideration of cost, time, and rare safety factors.
Some urgent care facilities now offer MRI capability, but it depends on the specific location. Urgent care MRI works well for acute orthopedic injuries (suspected ligament tears, knee or shoulder problems), some neurological symptoms without emergency signs, and straightforward single-question imaging. Hospital MRI remains appropriate for complex cases, suspected emergencies, multi-modality workups, and situations where the clinical picture isn’t yet clear. Check availability with the specific urgent care location.
Tesla (T) measures the magnetic field strength. 1.5T and 3T are both clinical-grade, with 3T being twice as powerful as 1.5T. The 3T produces higher-resolution images, shorter scan times, and better detail for neurological, musculoskeletal, and cardiac imaging. The 1.5T works well for routine imaging and some pediatric cases. Both fields are clinically used; the choice depends on the specific clinical question and any patient-specific factors like implants or claustrophobia tolerance.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo