How Integrated RIS PACS Synchronization Drives Revenue

Radiology Information Systems (RIS) and Picture Archiving and Communication Systems (PACS) are treated as line items on expense reports in most boardrooms. The integrated RIS PACS are viewed as necessary overhead—”the cost of doing business.”
This is a fundamental misunderstanding of the modern radiology business model.
Your imaging software is not just a digital filing cabinet; it is the engine of your Revenue Cycle Management (RCM). When your RIS and PACS are perfectly synchronized, they stop being cost centers and become profit drivers. Conversely, when they fail to communicate, they leak revenue through claim denials, increased Turnaround Time (TAT), and administrative friction.
This guide explores the financial impact of interoperability and how optimizing your workflow economics can directly impact your bottom line.

The Hidden Cost of “Swivel-Chair” Interoperability
Like other differences between RIS vs PACS, administrative staff often work in the RIS while clinical staff work in the PACS in a disjointed environment. Bridging this gap manually—typing patient IDs, copy-pasting reports—creates what we call “Swivel-Chair” interoperability.
This is not just annoying; it is expensive.
- The Cost of Data Entry Errors: A simple typo in a patient’s Date of Birth during manual entry can lead to an immediate claim denial from the payer.
- The Cost of Lost Orders: Without brokerless integration, orders can fail to cross from the RIS to the modality. This leaves machines idle and technicians wasting billable hours troubleshooting IT issues instead of scanning patients.
The Fix: Automated and integrated RIS PACS synchronization ensures that the demographic data in the billing claim matches the clinical data in the image header perfectly, reducing administrative overhead and denial rates.
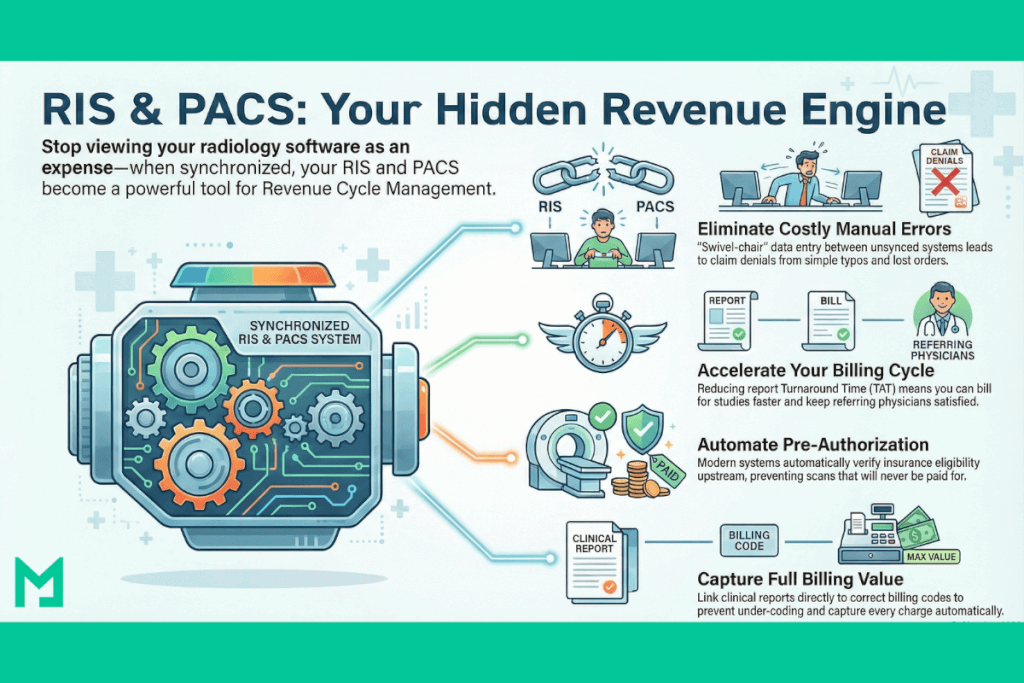
Speed Equals Revenue: Reducing Turnaround Time (TAT)
In radiology, time is inventory. The faster a study moves from “Scheduled” to “Finalized,” the quicker you can bill for it.
- Report Distribution Turnaround: Referring physicians are your customers. If they have to wait 48 hours for a report because your PACS doesn’t automatically trigger a fax/email via the RIS, they will send their next patient to your competitor.
- The “Stat” Bottleneck: In emergency cases, manual workflows slow down critical care.
By utilizing a Hybrid PACS Architecture, you ensure that large datasets (like 3D Mammography) load instantly for the radiologist. This technical speed translates directly to operational speed, allowing you to process more volume with the same staff.
Pre-Authorization and Eligibility: Stopping Leaks Upstream
Revenue leakage often happens before the patient even walks in the door.
Modern RIS-PACS platforms are moving beyond simple scheduling. They are integrating Eligibility Verification and Pre-Authorization bots directly into the workflow.
- The Old Way: A receptionist spends 20 minutes on hold with an insurance company to verify if an MRI is covered.
- The New Way: The system queries the payer API automatically when the order is placed. If authorization is missing, the system flags the patient before the scan is performed.
This prevents the worst-case scenario: performing an expensive high-tech scan that you can never collect payment for.
Automating Billing Codes (CPT/ICD-10)
The handoff between the Radiologist (Clinical) and the Coder (Financial) is a critical friction point.
If a radiologist dictates a complex study but the RIS doesn’t capture the specific protocol, the coder might downcode the exam to a lower reimbursement level.
- Structured Reporting: By using Structured Reporting templates within the PACS, you can ensure that the clinical findings automatically map to the correct CPT codes.
- Automated Charge Capture: When the study is marked “Final,” the PACS should instantly send an HL7 message to the RIS to drop the charge. No manual “superbills,” no lost charges.
The Medicai Advantage on Integrated RIS PACS Revenue Generation
Most legacy systems require expensive “interface engines” to translate between your RIS and PACS, adding annual maintenance costs and latency.
Medicai is different. We act as a Unified Data Layer. Because our VNA is built on API-first architecture, we don’t just “store images”—we act as the central clearinghouse that ensures your Billing Data (RIS) and Clinical Data (PACS) are identical.

- Faster Revenue Cycle: Our automated webhook triggers reduce the time from “Report Signed” to “Bill Sent” from hours to seconds.
- Zero Interface Costs: Eliminate the $15k/year maintenance fees for 3rd-party interface engines.
Investing in Efficiency
When evaluating a new software stack, do not just look at the license fee; consider the Operational ROI.
Ask your vendor:
- “Will this system reduce my claim denial rate?”
- “Will it automate my report distribution?”
- “Does it support HL7 FHIR to connect seamlessly with my billing provider?”
In 2025, the most profitable clinics are not the ones with the most expensive scanners; they are the ones with the most efficient data pipelines.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo