Radiologist Burnout: What Imaging Center Operators Can Actually Do About It

When a radiologist leaves a practice, the replacement cost — recruitment, credentialing, onboarding, and productivity ramp-up — is estimated at $500,000 to $1,000,000 per physician according to the American College of Radiology. That is the number an imaging center operator needs to hold in mind before any conversation about radiologist burnout. Burnout is not primarily a wellness problem to be managed with resilience programs and mindfulness apps. It is a workforce stability problem with a measurable financial consequence — and it is one that administrators have substantially more influence over than the conventional framing of “physician wellness” suggests.
The causes of radiologist burnout are substantially workflow-driven. Workflow is something administrators control. The technology infrastructure that supports or hinders the reading workflow is something administrators procure. The scheduling model that determines whether radiologists cover overnight shifts is designed by administrators. Understanding which burnout drivers fall within the administrator’s sphere of influence — and acting on them systematically — is the most impactful step an imaging center operator can take to address a problem that is measurably worsening.
The Numbers — What the Research Actually Shows
The burnout statistics cited across radiology literature vary depending on the measurement instrument used, the population surveyed, and the year of data collection. The following are the primary sourced figures that this post and the Medicai blog use as reference data.
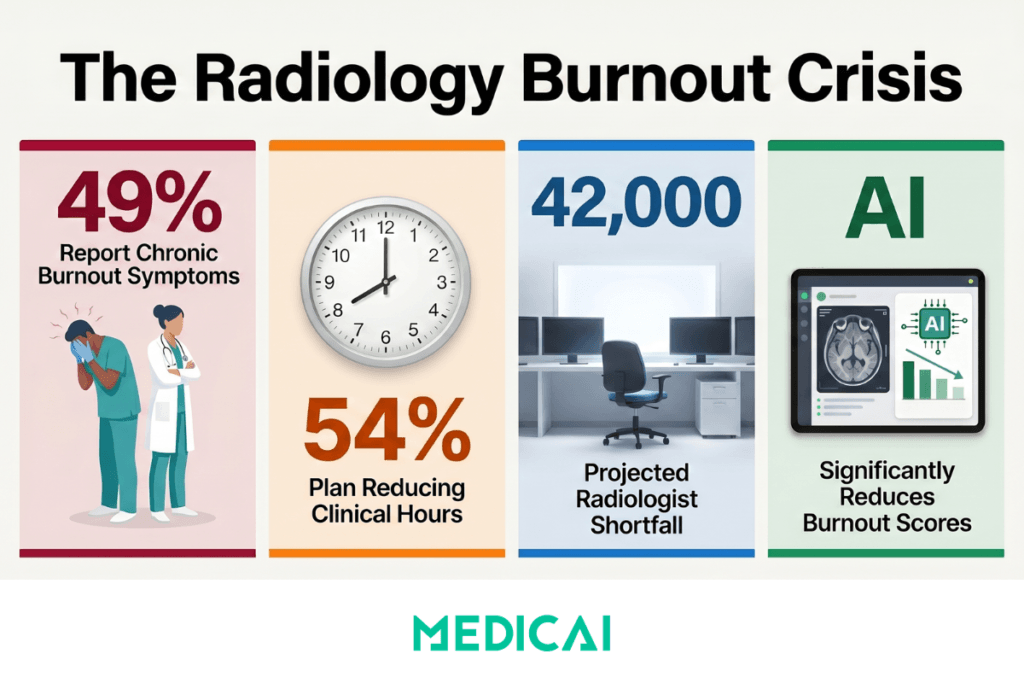
49% of radiologists report burnout symptoms. The 2023 Medscape Physician Burnout and Depression Report — the largest annual survey of US physician burnout, covering 9,175 physicians across 29 specialties — found that 49% of radiologists reported burnout symptoms. The Medscape survey uses a validated self-report methodology aligned with the Maslach Burnout Inventory framework, assessing emotional exhaustion, depersonalization, and reduced sense of personal accomplishment. Radiology ranked in the top third of specialties by burnout prevalence in the 2023 report.
Pooled prevalence of 40–50% across the published literature. A 2023 systematic review — “Incidence and factors associated with burnout in radiologists” (PMC10618688) — analyzed 38 studies covering 9,428 radiologists and found burnout prevalence ranging from 15% to 75% depending on the measurement instrument used. The pooled estimate across studies using the Maslach Burnout Inventory or equivalent validated instruments was 40–50%. The variability reflects differences in measurement methodology, not variability in the underlying phenomenon.
54% of radiologists plan to reduce clinical hours within three years. The ACR Bulletin “Burnout Fueling Workforce Woes” reported that 54% of radiologists surveyed indicated plans to reduce clinical hours within three years — a forward-looking workforce capacity indicator directly linked to burnout in the underlying survey data. For an administrator planning staffing levels, this figure means more than the prevalence rate: it represents the proportion of the current workforce that is actively planning to deliver fewer hours of clinical output.
AI workflow tools are associated with measurable burnout reduction. A 2024 study published in JAMA Network Open — “Artificial Intelligence and Radiologist Burnout” — found that radiologists using AI-assisted workflow tools showed statistically significant reductions in burnout scores compared to a control group using standard reading workflows. The mechanism was cognitive load reduction rather than volume increase — the AI handled triage, prioritization, and structured template population, allowing radiologists to concentrate on interpretation.
The radiologist shortage amplifies everything. The Neiman Health Policy Institute’s 2024 workforce projections — published in the Journal of the American College of Radiology — project a shortfall of 42,000 full-time equivalent radiologists in the United States by 2055 under base-case demand growth assumptions. Burnout-driven early retirement and career exit are modeled as significant contributors to the supply deficit. A practice that loses a radiologist to burnout-driven career exit is competing for a replacement in a market that is structurally and increasingly undersupplied.
What Actually Causes Radiologist Burnout — and What Administrators Control
The most important distinction in any burnout analysis is between the causes administrators can influence and those they cannot. Most burnout discussions treat the causes as fixed features of the specialty — the inherent demands of diagnostic radiology are presented as the primary driver, with administrators positioned as helpless observers of a phenomenon driven by specialty-intrinsic factors. The research literature does not support this framing.
The Medscape 2023 report found that “too many bureaucratic tasks” was the number one cited burnout contributor among radiologists — ahead of “too many hours,” “lack of respect from colleagues,” and “insufficient compensation.” Bureaucratic tasks in a radiology reading environment are almost entirely administrator-designed processes: prior authorization workflows, report formatting mandates, billing documentation requirements, and the number of systems a radiologist must interact with to complete a single reading cycle.
Within administrator control
Study volume and reading pace pressure. A 2022 paper in Academic Radiology found that radiologists who read more than 80 studies per shift reported burnout scores 2.3 times higher than those who read fewer than 50 studies per shift, after controlling for subspecialty, practice type, and years of experience. The mechanism is not simply fatigue from volume — it is the cognitive burden of continuous high-stakes decision-making under time pressure without recovery intervals. Administrators who set productivity targets based on RVU maximization without accounting for cognitive load accumulation are directly contributing to the conditions that lead to burnout.
Administrative and non-interpretive workflow burden. Every system the radiologist must log into, every form they must complete, every non-interpretive step in the reading workflow — prior study retrieval, report template selection, manual measurement entry, billing documentation — is an administrator-designed or administrator-procured process. Medscape data consistently identify this category as the primary modifiable driver of burnout.
Technology adequacy. Radiologists using outdated PACS interfaces, slow image loading, poorly configured hanging protocols, and manual prior study retrieval report significantly higher burnout prevalence than those using optimized digital workflows. This is a direct administrative investment decision. Technology that creates friction in the reading workflow is not a neutral factor — it is a burnout accelerant that the administrator chose through a procurement decision.
On-call and overnight coverage obligations. The PMC systematic review identified on-call obligations and overnight coverage requirements among the strongest single predictors of burnout in the literature. A scheduling model that requires in-house radiologists to cover overnight shifts after a full day reading schedule is a structural burnout accelerant. It is also one that teleradiology infrastructure directly addresses — by distributing overnight coverage across a geographically distributed reading panel rather than requiring in-house rotations.
Schedule control and subspecialty alignment. Radiologists who read within their subspecialty training and have meaningful input into their scheduling report lower burnout prevalence across multiple studies. Mixed-modality reading schedules that alternate between complex subspecialty cases and simple general studies maximize cognitive context-switching overhead without increasing diagnostic output.
Outside administrator control
The inherent cognitive demands of diagnostic radiology — sustained attention, high-stakes pattern recognition under time pressure, and the medico-legal weight of every signed report — are intrinsic to the specialty. The emotional burden of communicating adverse findings is similarly intrinsic. These factors contribute to burnout risk in radiology compared with other physician specialties and cannot be eliminated through workflow or administrative interventions. Administrators who conflate these immutable demands with the modifiable workflow factors above consistently underestimate their own capacity to reduce burnout — and consistently underinvest in the workflow changes that would produce measurable improvement.
How Administrators Identify Burnout Before It Becomes Attrition
Radiologists are among the physician specialties least likely to self-report burnout to a supervisor. The culture of self-sufficiency in medicine, the perceived career risk of disclosing struggle, and the gradual onset of burnout symptoms — which are partially normalized in high-volume reading environments — all contribute to a detection gap. By the time a radiologist verbally signals that they are struggling, they are often already planning to leave. The interval between the onset of clinically significant burnout and the departure notification averages 12 to 18 months in the physician burnout literature — a window during which the administrator has repeated opportunities to intervene if they are looking at the right signals.
Productivity baseline deviation. A radiologist who historically reads 65 studies per shift and sustains 48 per shift over 8 or more weeks is not necessarily slower — they may be spending more time per study due to indecision, double-checking behavior, and difficulty concentrating under cognitive depletion. A productivity decline of 15–20% from personal baseline, sustained over two or more months, is a leading indicator worth a direct conversation. It is not a performance management trigger — it is a welfare signal.
Turnaround time variance. Burnout is associated with increased variability in TAT rather than consistently slower TAT. A radiologist reading in a normal cognitive state produces TATs that cluster predictably around their personal range. A burnout-affected radiologist produces unpredictably fast TATs — tasks completed quickly with reduced attention — and unpredictably slow tasks in which concentration is particularly compromised. A widening TAT variance signature, visible in PACS analytics, is a more sensitive indicator of burnout than average TAT alone.
Addendum and correction rate increase. Burnout is associated with increased reporting errors — not from carelessness but from the cognitive depletion that characterizes Stage 2 and Stage 3 burnout as defined by the Maslach Burnout Inventory. An increase in addendum rate or correction requests not explained by a change in study complexity or case mix is a signal worth investigating as a welfare issue, not a quality management issue.
Leave pattern changes. The Medscape report found that burnout-affected physicians took an average of 4.2 more sick days per year than non-burnout colleagues in the year preceding career exit. Sick leave pattern changes are visible in scheduling systems and can be tracked without any clinical data access.
Withdrawal from non-clinical activities. Radiologists who previously participated in departmental education, quality improvement projects, peer consultation, or case conferences and who progressively disengage from these activities are showing the depersonalization dimension of burnout — the stage in which emotional investment in the work and the institution begins to visibly reduce. This is not a performance issue. It is the clearest behavioral signal available to an administrator before the resignation conversation.
Five Levers Imaging Center Operators Can Actually Pull
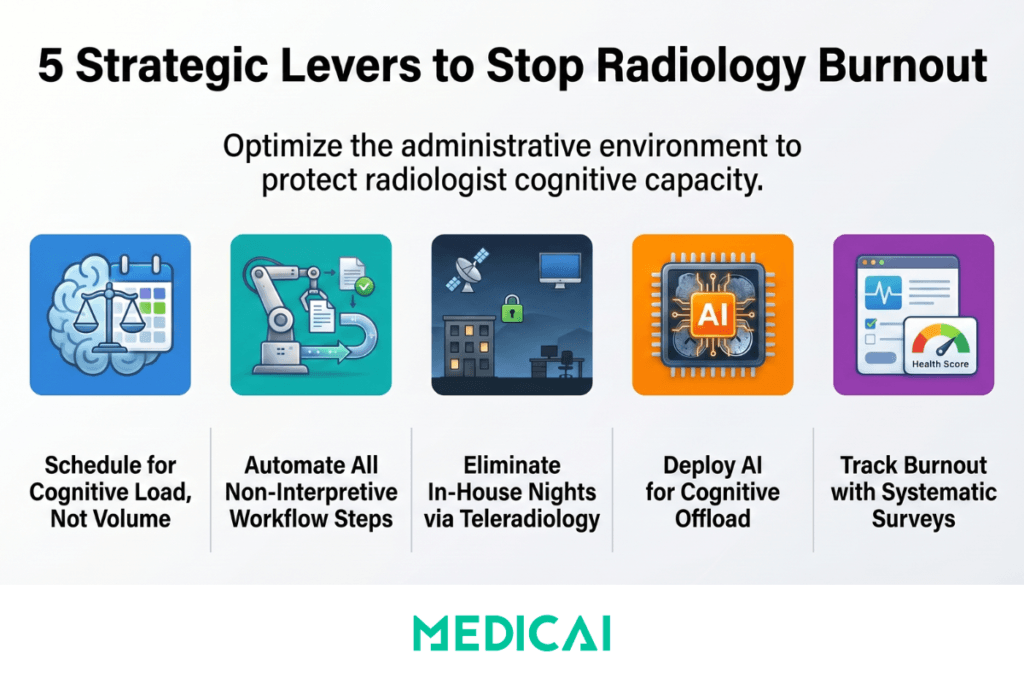
Lever 1 — Redesign reading schedules around cognitive load, not RVU targets
A 2019 paper in RSNA RadioGraphics identified approximately 40 minutes of continuous reading as the threshold beyond which error rates begin to increase significantly — consistent with broader cognitive fatigue research across attention-demanding professional tasks. The administrative implication is direct: reading schedules designed to maximize RVU production per shift, without mandatory recovery intervals, simultaneously reduce diagnostic accuracy and increase burnout risk. The two outcomes are not in tension — they are the same outcome measured by different instruments.
Practical implementation does not require reducing total reading volume. Scheduled 10-minute breaks every 45–60 minutes of continuous reading — enforced in the schedule rather than left to the individual radiologist’s discretion — maintain total productivity while reducing the error rate accumulation and cognitive exhaustion that drive burnout. Protected intervals for non-reading tasks (education, peer consultation, quality improvement) provide cognitive recovery without requiring the radiologist to disengage from the department. Subspecialty grouping of worklists so radiologists read within their area of highest competency for defined blocks — rather than alternating between complex subspecialty and routine general studies in a volume-maximizing random order — reduces the context-switching overhead that contributes to cognitive fatigue.
Lever 2 — Eliminate non-interpretive reading workflow steps
The most impactful single administrative action available to most imaging centers is to audit the non-interpretive steps in the reading workflow and eliminate those that can be automated. Non-interpretive steps — prior study retrieval, viewport arrangement, window and level adjustment, report template selection, manual measurement entry, structured field completion — are not the work radiologists are trained to do. They are the overhead surrounding the work radiologists are trained to do. In a 65-study reading shift, 45 seconds of non-interpretive setup overhead per study represents 49 minutes of accumulated non-interpretive time — time spent on mechanical tasks in exactly the conditions that produce the “bureaucratic burden” category the Medscape data identifies as the primary burnout driver.
Hanging protocol configuration that eliminates manual viewport arrangement and prior study retrieval — covered in detail in the radiology hanging protocols guide — addresses the viewer configuration dimension of this overhead. Structured reporting with AI-assisted dictation that populates template fields from dictated text, proposes classification system categories from extracted measurements, and delivers the completed report to the EHR through an automated HL7 workflow — covered in the structured radiology reporting guide — addresses the reporting dimension. Together, these two workflow optimizations address the modifiable administrative burden that the Medscape data consistently identify as the number one burnout driver.
Lever 3 — Use teleradiology to eliminate in-house overnight coverage obligations
The on-call and overnight coverage obligation is one of the strongest single predictors of burnout in the PMC systematic review. A radiologist who covers a full day reading schedule and then takes an in-house overnight shift is not simply working more hours — they are disrupting sleep, compressing physiological recovery time, and accumulating cognitive debt that measurably impairs next-day reading performance. The cumulative effect of irregular on-call scheduling over months is evident in burnout scores long before it appears in resignation letters.
Teleradiology infrastructure — a cloud PACS with a zero-footprint browser viewer that allows any credentialed radiologist to read any study from any location — enables distributing overnight coverage across a geographically distributed reading panel rather than requiring in-house radiologists to rotate overnight shifts. For a four-radiologist group, eliminating in-house overnight coverage through a teleradiology arrangement reduces each radiologist’s on-call burden from 1 in 4 overnight shifts to 0 in-house overnight obligations. The TAT and coverage requirements are met by the teleradiology arrangement. The in-house team reads only during standard hours.
This is the greatest single-impact structural change available to most small and mid-size radiology groups, and it requires cloud PACS infrastructure to implement. The same infrastructure that enables remote reading in a teleradiology model also eliminates the in-house overnight obligation for practices that deploy it — a direct burnout-reduction mechanism built into the infrastructure decision.
Lever 4 — Deploy AI as a cognitive offload mechanism, not a productivity multiplier
The 2024 JAMA Network Open study found that AI-assisted workflow tools reduced burnout scores — but the mechanism matters for how administrators implement them. AI reduced burnout not primarily by increasing the number of studies read per shift — the productivity framing most vendors lead with — but by reducing the cognitive load per study. Specifically, AI handled triage and prioritization decisions, flagged studies requiring immediate attention, and populated structured report templates from dictated text. These are the mechanical and administrative functions that the Medscape data identifies as the primary drivers of burnout, and AI tools address them directly when configured and communicated as cognitive offload tools rather than throughput accelerators.
An administrator who implements AI tools with a message of “now you can read 20% more studies” is adding workload while appearing to help. An administrator who implements the same tools with a message of “this handles the routine so you can concentrate on the complex” is reducing cognitive burden while achieving the same productivity outcome. The technology is identical. The burnout trajectory depends entirely on how the administrator frames and implements the change — and whether the productivity gain is absorbed by the practice or returned to the radiologist as reduced per-study cognitive overhead.
AI-assisted structured reporting — the specific tool that eliminates per-report formatting burden — is covered in the structured radiology reporting guide. The cognitive offload framing described here is the correct implementation context for that tool in a burnout reduction program.
Lever 5 — Measure burnout systematically rather than assuming you would notice
The most consistent finding in the physician burnout literature is that clinician burnout is significantly underdetected by supervisors and administrators until the stage where career exit is already being planned. Observation-based detection — noticing that a radiologist seems less engaged, reads more slowly, or calls in sick more often — catches burnout late in its progression, when intervention is most difficult, and attrition is most likely.
The Maslach Burnout Inventory — the gold standard validated instrument for physician burnout assessment — takes approximately 15 minutes to complete and produces scores on three dimensions: emotional exhaustion, depersonalization, and personal accomplishment. A semi-annual, anonymous MBI survey administered to all radiologists in the practice provides the administrator with a leading indicator of burnout risk that is more reliable, earlier, and more actionable than any observation-based detection system. The ACR’s Radiology Leadership Institute provides burnout assessment resources and benchmarking data specifically calibrated for radiology practice contexts.
The measurement must be followed by visible action. An administrator who measures burnout and takes no action in response to the results produces worse outcomes than one who does not measure at all — because the survey process itself raises expectations that the practice leadership cares about the result. When those expectations are disappointed, trust erodes, and the burnout-to-attrition timeline accelerates. The survey is the beginning of the program, not its end.
The Technology Stack That Supports Burnout Reduction
The five levers described above require operational decisions — schedule redesign, workflow audit, staffing model change, AI implementation, and measurement program. Three of the five depend on having the right technology infrastructure in place. An administrator who wants to eliminate in-house overnight coverage needs a cloud PACS that supports remote reading. An administrator who wants to eliminate non-interpretive workflow overhead needs a PACS with configurable hanging protocols and an integrated structured reporting platform. An administrator who wants to deploy AI as a cognitive offload tool needs a reporting platform with AI-assisted dictation and NLP-based template population.
Medicai’s cloud-native PACS on Microsoft Azure provides the infrastructure layer that connects all three: a zero-footprint browser-based DICOM viewer with configurable hanging protocols for per-study-type display optimization, a structured reporting module with AI-assisted dictation and automated HL7 report distribution, and a teleradiology architecture that enables remote reading from any device without VPN or thick-client installation. For practices evaluating whether their current technology stack is contributing to the modifiable burnout drivers described in this post, the free 14-day trial provides a full workflow comparison against the current reading environment.
The connection between technology infrastructure and burnout is not theoretical. The 2024 study in JAMA Network Open found statistically significant reductions in burnout scores among radiologists using AI-assisted workflow tools. The mechanism — cognitive load reduction through automation of non-interpretive tasks — is precisely what the structured reporting and hanging protocol optimizations described in this post deliver. The administrator’s job is to ensure the infrastructure enables those reductions and to frame the implementation so the cognitive benefit returns to the radiologist rather than being converted into additional throughput demand.
Frequently Asked Questions
What is the burnout rate for radiologists?
The 2023 Medscape Physician Burnout and Depression Report found that 49% of radiologists reported burnout symptoms, placing radiology in the top third of specialties by burnout prevalence. A 2023 systematic review published in PMC (PMC10618688) analyzed 38 studies covering 9,428 radiologists and found a pooled prevalence of 40–50% using validated measurement instruments. The ACR Bulletin “Burnout Fueling Workforce Woes” reported that 54% of radiologists planned to reduce clinical hours within three years — a forward-looking workforce capacity indicator linked to burnout in the underlying survey data. These three figures come from different measurement approaches and should not be averaged — each captures a different dimension of the same problem.
What causes radiologist burnout?
The Medscape 2023 report identified “too many bureaucratic tasks” as the number one cited burnout contributor among radiologists — ahead of hours, compensation, and lack of respect. In radiology, this category includes prior authorization burden, report formatting requirements, non-interpretive reading workflow overhead, and administrative documentation demands. Secondary causes with strong research support include excessive study volume without recovery intervals, on-call and overnight coverage obligations, schedule inflexibility, and inadequate technology that creates friction in the reading workflow. The inherent cognitive demands of diagnostic radiology — sustained attention, high-stakes pattern recognition, medico-legal weight of every signed report — are intrinsic to the specialty and contribute to baseline burnout risk. Still, they are not the primary modifiable drivers identified in the literature.
How does AI reduce radiologist burnout?
The 2024 JAMA Network Open study “Artificial Intelligence and Radiologist Burnout” found that AI-assisted workflow tools led to statistically significant reductions in radiologists’ burnout scores. The mechanism was cognitive load reduction rather than volume increase: AI handled triage and study prioritization, flagged urgent findings, and populated structured report template fields from dictated text — reducing the administrative and mechanical overhead per study without changing the interpretive demand. The key implementation variable is framing: AI tools deployed as throughput accelerators (“read more studies”) do not reduce burnout. AI tools deployed as cognitive offload mechanisms (“concentrate on the complex cases”) do.
What is the radiologist shortage, and how does burnout connect to it?
The Neiman Health Policy Institute’s 2024 projections forecast a shortfall of 42,000 full-time equivalent radiologists in the United States by 2055, rising to 95,000 FTE under higher growth scenarios for imaging utilization. The shortage is driven by a combination of insufficient training pipeline volume — the number of radiology residency positions has not kept pace with demand growth — and active workforce attrition. Burnout contributes to the attrition side of the equation in two ways: it drives experienced radiologists to reduce their clinical hours (as reported by 54% of radiologists in the ACR Bulletin survey) and to exit clinical practice earlier than planned. A practice that loses a radiologist to burnout-driven career exit is recruiting in a market that is structurally undersupplied and becoming more so.
What can radiology administrators do about burnout?
Five levers with strong research support are within the administrator’s direct control. First, redesign reading schedules around cognitive load rather than RVU maximization — mandatory recovery intervals and subspecialty-aligned worklist grouping reduce cognitive fatigue accumulation without reducing total output. Second, audit and eliminate non-interpretive reading workflow steps through hanging protocol optimization and AI-assisted structured reporting. Third, use teleradiology infrastructure to distribute overnight coverage across a remote reading panel rather than requiring in-house overnight rotations. Fourth, deploy AI workflow tools as cognitive offload mechanisms rather than throughput multipliers — the framing of implementation determines whether the same technology reduces or maintains burnout. Fifth, measure burnout systematically with validated instruments such as the Maslach Burnout Inventory on a semi-annual basis, and take visible action on the results.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo