Ophthalmology PACS: Cloud Imaging Software for OCT, Fundus, and Retinal Workflows

Ophthalmology PACS is the imaging IT platform that captures, stores, retrieves, and shares the diagnostic images ophthalmology practices generate — optical coherence tomography (OCT) volumes, fundus photographs, slit lamp images, anterior segment photography, and retinal angiography. The software replaces the per-device storage that historically lived inside each imaging instrument (OCT scanner, fundus camera, slit lamp) with a centralized archive accessible from any authorized workstation, integrates with ophthalmology EHR systems for chart-in-context viewing, and increasingly supports multi-site practices through cloud-based deployment. Modern ophthalmology PACS handles the full imaging workflow from acquisition through reading to long-term retention without the legacy IT infrastructure that single-device archives required.
What ophthalmology PACS does
Ophthalmology PACS handles three operational functions: image acquisition from the practice’s imaging hardware (OCT scanners, fundus cameras, slit lamp imaging systems, anterior segment cameras, retinal angiography units, visual field analyzers), centralized storage and indexing of those images across patient visits, and viewer access from any authorized workstation in the practice.
The architectural choice that defines modern ophthalmology PACS is vendor-neutral image handling. Historically, each ophthalmology imaging device shipped with its own proprietary software — Zeiss Forum for Cirrus OCT data, Heidelberg HEYEX for Spectralis, Topcon IMAGEnet for Triton — each writing to its own format and producing its own viewer. A clinician working across multiple devices in the same practice had to learn five different interfaces and accept that each device’s data lived in its own silo. Vendor-neutral ophthalmology PACS resolves this by ingesting data from any DICOM-compliant device, normalizing it to a single archive, and presenting it through a single viewer.
The operational driver behind centralization is the OCT file size. A single OCT volume runs 100 to 500 MB. A busy ophthalmology practice generates 50 to 100 OCT scans per day across glaucoma management, retinal disease, and diabetic retinopathy follow-up. The cumulative daily storage burden — 5 to 50 GB across ophthalmology imaging modalities — makes per-device archives operationally impractical past a certain practice size, particularly for multi-clinic operations.
Ophthalmology imaging modalities that the PACS supports
Ophthalmology PACS supports six primary imaging modalities, each with distinct file formats, file sizes, and clinical workflow patterns. The diversity is part of what makes ophthalmology imaging operationally complex — a single patient encounter may generate data from three or four different modalities, each contributing to a complete diagnostic picture.
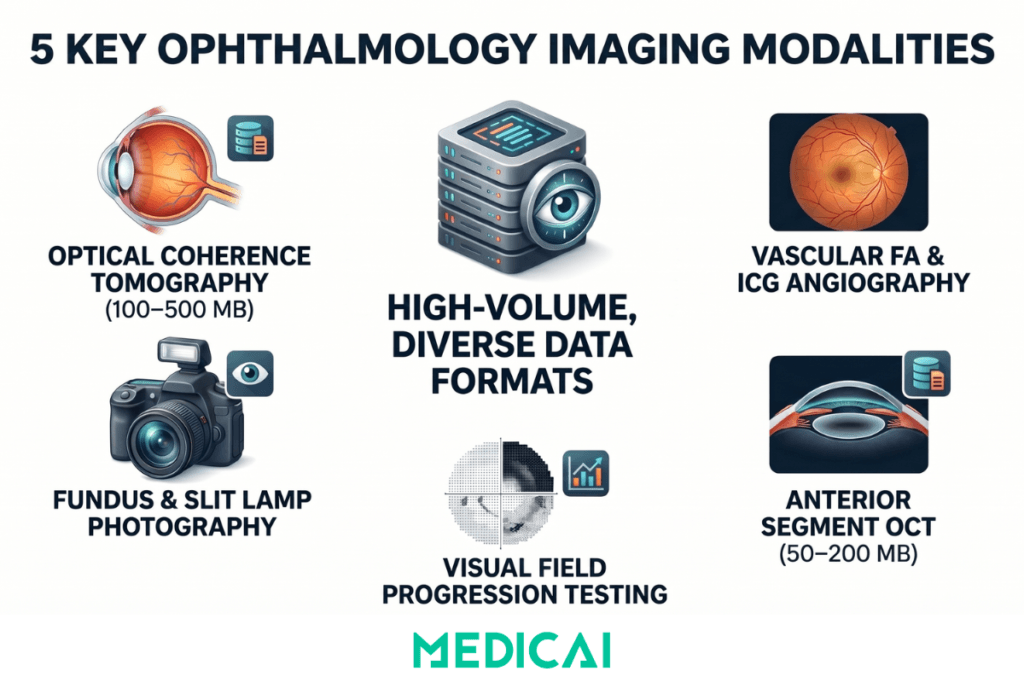
- Optical coherence tomography (OCT) is the dominant imaging modality in modern ophthalmology. OCT produces 3D cross-sectional images of the retina and anterior segment using low-coherence interferometry, allowing measurement of retinal layer thickness, optic nerve head morphology, and macular structure. OCT volumes run 100 to 500 MB per scan and are central to glaucoma management (RNFL thickness tracking), diabetic retinopathy monitoring (macular edema quantification), and macular degeneration follow-up (subretinal fluid measurement). OCT storage is the primary driver behind cloud adoption in ophthalmology.
- Fundus photography captures color photographs of the retina. Modern fundus cameras produce digital images at 5 to 20 MB per photograph, used for diabetic retinopathy screening, macular degeneration documentation, optic disc evaluation, and hypertensive retinopathy assessment. Volume is moderate — typically 1 to 5 images per affected patient visit.
- Fluorescein angiography (FA) and indocyanine green (ICG) angiography are vascular imaging studies using intravenous contrast agents. Each study captures a sequence of timed images (transit phase, mid phase, late phase) totaling 50 to 150 MB. Used primarily for retinal vascular disease — diabetic retinopathy, retinal vein occlusion, age-related macular degeneration, and central serous chorioretinopathy.
- Slit lamp imaging captures anterior segment photographs of the cornea, conjunctiva, anterior chamber, and lens. File sizes are small (2 to 10 MB per image), but volume is high in cataract and corneal practices, where slit lamp documentation supports preoperative planning and longitudinal disease tracking.
- Anterior segment OCT images the cornea, anterior chamber angle, and crystalline lens at 50-200 MB per scan. Used in glaucoma evaluation (angle assessment), refractive surgery planning (corneal pachymetry mapping), dry eye management (tear film analysis), and contact lens fitting.
- Visual field testing (Humphrey, Octopus) produces small file sizes but high frequency — used quarterly to monthly for glaucoma progression monitoring, neurological assessment, and ocular hypertension follow-up. Modern PACS systems integrate visual field data alongside imaging to support side-by-side progression review.
Ophthalmology PACS integration with EHR systems
Ophthalmology PACS doesn’t operate in isolation. It integrates with the practice’s ophthalmology EHR system so that imaging studies appear in context within the patient’s clinical record, rather than as a separate, parallel system the clinician has to log into.
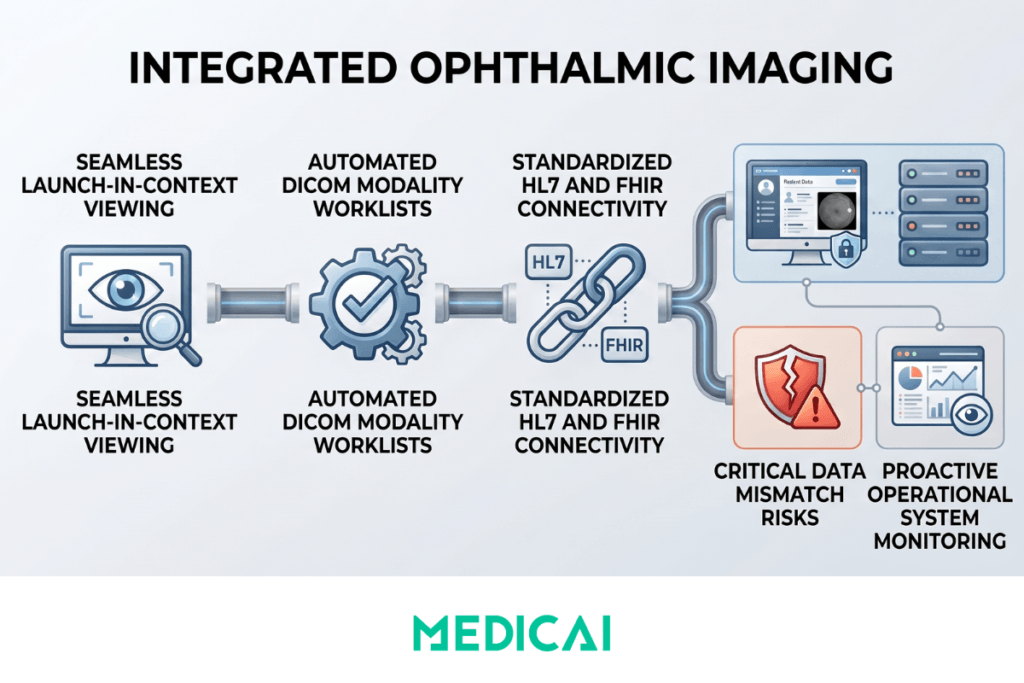
The major ophthalmology-specific EHR platforms — NextGen Healthcare, ModMed (Modernizing Medicine), Compulink, RevolutionEHR, Nextech, and EyeMD EMR — each support some combination of integration protocols. HL7 v2 messaging carries patient demographics, encounter information, and order routing between the EHR and PACS. FHIR APIs increasingly carry the same information in modern cloud-native deployments. DICOM modality worklist (MWL) carries the scheduled imaging context from the EHR to the imaging device, so when a technician brings up a patient on the OCT scanner, the scheduled exam appears automatically rather than requiring manual entry.
The integration goal is launch-in-context viewing. When the ophthalmologist opens a patient’s chart in the EHR, the imaging studies appear inline — either as embedded thumbnails that the clinician can expand, or as a button that launches the PACS viewer pre-populated to the relevant patient and study set. This eliminates the legacy workflow in which clinicians had to log in to a separate PACS application, search for the patient, and then return to the EHR to dictate findings.
What breaks ophthalmology EHR-PACS integration most often: patient ID mismatches between the EHR and the imaging archive (caused by demographic updates that propagate unevenly), accession number drift when orders get canceled and rebooked, and MWL outage at the imaging device that forces manual data entry — which then creates orphan studies that the PACS can’t reconcile to an order. Each of these failure modes is manageable with monitoring and reconciliation workflows, but absent that operational discipline, the integration silently degrades over time.
Cloud vs on-premise ophthalmology PACS deployment
Ophthalmology PACS runs on one of two architectures: a local server in each practice or a centralized cloud archive accessed over secure HTTPS. The choice has cascading consequences for OCT storage scaling, multi-site capability, EHR integration overhead, and disaster recovery.
For ophthalmology practices specifically, OCT file sizes drive the deployment decision more than any other factor. A practice running 50 to 100 OCT scans per day across glaucoma, retinal, and diabetic retinopathy patients generates 5 to 50 GB of new imaging data daily. Over a 7- to 10-year retention period, the cumulative archive can reach hundreds of terabytes. On-premise deployments require explicit capacity planning, hardware refresh cycles, and IT staff to manage backup and retrieval. Cloud deployments handle the same data growth through automated lifecycle policies that tier data into hot, warm, and cold states without operational intervention.
| Dimension | On-premise ophthalmology PACS | Cloud-based ophthalmology PACS |
|---|---|---|
| Infrastructure | Local server in practice; hardware refresh every 5 to 7 years; IT staff required for maintenance | Vendor-managed cloud archive; no on-premise hardware; no refresh cycle |
| OCT storage scaling | Manual capacity planning as OCT volume grows; hardware upgrades for storage expansion | Elastic cloud storage scales automatically with OCT volume; hot/warm/cold tiering by access pattern |
| Multi-site access | Each clinic operates in isolation; specialists travel or use screen-sharing for cross-site cases | Centralized archive accessible from any clinic; specialists review remotely from anywhere in the network |
| EHR integration | Per-clinic EHR-PACS integration setup required; network outages and firewall changes break message routing | Cloud-native API integration; single integration scales across all clinics |
| Disaster recovery | Local backup discipline required to test restores; ransomware risk significant without rigorous protocols | Geo-redundant cloud replication across regions; survives clinic-level fire, flood, or ransomware |
| Best fit | Single-clinic deployments with low OCT volume and strong on-site IT | Multi-clinic practices, OCT-heavy practices, practices using remote specialists |
The decision between on-premise and cloud-based ophthalmology PACS is no longer a pure IT architecture choice — it’s a growth-strategy decision. Single-clinic deployments with stable OCT volume and dedicated on-site IT can run on-premise indefinitely without operational pain. The moment any of those assumptions change — opening a second location, adding a retinal subspecialist who works remotely, expanding into wide-field OCT imaging that doubles file sizes — the cloud-native model becomes structurally advantageous. For practices considering OCT for the first time, the storage and bandwidth requirements of 3D imaging often make cloud-based deployment the default rather than the upgrade.
Multi-site ophthalmology practice considerations
Multi-site ophthalmology practices face operational realities that single-clinic deployments don’t encounter. The same architectural choice that’s a preference question for a single practice becomes a structural constraint on growth for a group operating 5, 20, or 100 clinics.
Floating clinicians need network-wide imaging access. Associate optometrists and retinal subspecialists who rotate across clinics can’t be expected to log into each clinic’s local PACS separately or carry imaging data on portable devices. They need a single login that surfaces the complete imaging history for the relevant patient, regardless of which clinic in the network captured the studies.
Referring-specialist workflow accelerates dramatically with centralized imaging. A general ophthalmologist at one clinic referring a patient to a retinal subspecialist at another clinic shouldn’t need to print, burn, or email imaging studies — the subspecialist should be able to open the patient’s record and see the OCT volumes, fundus photographs, and prior-visit comparisons already there.
Centralized imaging review also supports quality assurance and clinical training. Senior clinicians can review questionable cases from associate clinicians across the network, ensuring diagnostic standards are met and identifying systematic teaching opportunities.
The integration that ties this together is ophthalmology practice management software. Multi-clinic practices typically run on Nextech, Eyefinity, ModMed, or similar platforms that need to surface imaging in context within the patient chart across the network. The economic case for cloud-native deployment compounds across these dimensions: cloud scales sublinearly with clinic count, while on-premise scales linearly with hardware, IT staff, and per-clinic integration overhead.
Medicai’s ophthalmology PACS solution
Medicai’s ophthalmology PACS solution addresses the architectural realities described above through cloud-native infrastructure built specifically for multi-modality, multi-site ophthalmology practices.
The vendor-neutral archive (VNA) layer ingests data from any DICOM-compliant ophthalmology imaging device, regardless of manufacturer — Zeiss Cirrus and Forum, Heidelberg Spectralis, Topcon Triton and Maestro, Optos wide-field, Nidek, and others — and normalizes the data into a single archive accessible through a single browser-based viewer. The viewer carries FDA diagnostic clearance, enabling clinicians to read from any authorized workstation, including remote locations and home offices.
Integration with ophthalmology EHR systems occurs via HL7 v2 messaging and FHIR APIs, enabling launch-in-context viewing within NextGen, ModMed, Compulink, RevolutionEHR, Nextech, and EyeMD EMR. Patient demographics, encounter context, and order routing flow between the EHR and the imaging archive without per-clinic custom integration engineering.
Multi-site support is built into the architecture rather than added as a feature — a practice operating one clinic or fifty clinics uses the same platform, with elastic storage scaling that adapts to growing OCT volume without manual capacity planning. HIPAA and GDPR compliance, encryption at rest and in transit, geo-redundant replication, and automated lifecycle management are baseline rather than upgrades.
To evaluate cloud-native ophthalmology PACS for a specific practice, explore Medicai’s ophthalmology PACS solution.
Where ophthalmology PACS is heading
Three trends are reshaping ophthalmology PACS through 2027 and beyond. The strategic question for practices evaluating PACS today is whether the chosen platform accommodates these changes or constrains them.
AI-augmented OCT analysis is moving from research to clinical practice. Tools now perform automated retinal layer segmentation, glaucoma progression detection, diabetic retinopathy grading, and macular fluid quantification. The next generation will integrate into the OCT acquisition workflow itself, flagging suspect findings before the clinician opens the study and pre-populating structured measurements into the report. PACS platforms that support AI orchestration at the workflow level will absorb these tools cleanly; platforms that don’t will require parallel infrastructure.
Telemedicine for ophthalmology is expanding beyond pilot deployments, particularly in diabetic retinopathy screening programs and underserved rural populations. Remote OCT and fundus interpretation requires a PACS architecture that supports browser-based reading from any authorized location without VPN overhead.
Cloud-native deployment is becoming the default rather than the upgrade for new practice deployments. The economic and operational case favors the cloud, particularly as OCT becomes the modality center of gravity and as multi-site practice models continue to consolidate the specialty.
Frequently asked questions about ophthalmology PACS
These eight questions cover the queries ophthalmology practice owners, IT directors, practice managers, and clinical leadership most often search for when evaluating ophthalmology PACS. Each answer is structured for direct citation in AI Overview and PAA boxes.
Ophthalmology PACS (Picture Archiving and Communication System) is the imaging IT platform that captures, stores, and shares the diagnostic images ophthalmology practices generate — OCT volumes, fundus photographs, slit lamp images, anterior segment photography, and retinal angiography. It centralizes images from multiple imaging devices into a single archive accessible from any authorized workstation and integrates with ophthalmology EHR systems for chart-in-context viewing.
Ophthalmology PACS handles the imaging archive — storage, retrieval, and viewing of diagnostic images. An ophthalmology EHR (Electronic Health Record) handles the clinical record — diagnoses, exam findings, prescriptions, notes, and patient history. The two systems integrate so that imaging appears in context within the patient’s chart, but they perform fundamentally different functions. Most practices operate with HL7 or FHIR integration.
Ophthalmology PACS supports six primary modalities: optical coherence tomography (OCT) for 3D retinal imaging, fundus photography for retinal color photographs, fluorescein and ICG angiography for vascular imaging, slit lamp imaging for anterior segment documentation, anterior segment OCT for corneal and anterior chamber imaging, and visual field testing for glaucoma monitoring. Modern PACS handles all modalities in a unified archive regardless of the imaging device manufacturer.
Yes. Modern ophthalmology PACS integrates with ophthalmology-specific EHR platforms (NextGen, ModMed, Compulink, RevolutionEHR, Nextech, EyeMD EMR) and practice management systems through HL7 messaging, FHIR APIs, or DICOM modality worklist. The integration enables launch-in-context viewing — clinicians open the patient chart in the EHR, and imaging studies appear inline rather than requiring a separate PACS login.
Cloud-based ophthalmology PACS fits practices with OCT-heavy imaging volume, multi-clinic operations, remote specialists, or plans for expansion — the cloud storage economics scale better with OCT file sizes, and the access model supports cross-site workflow. On-premise PACS still fits single-clinic deployments with low OCT volume and dedicated on-site IT. The decision is increasingly cloud-default as OCT becomes the dominant modality.
OCT volumes are 100-500 MB per scan — an order of magnitude larger than 2D fundus photographs (5-20 MB) or slit lamp images (2-10 MB). A busy ophthalmology practice generates 50-100+ OCT scans daily across glaucoma management, retinal disease, and diabetic retinopathy follow-up. The cumulative storage and bandwidth requirements push most multi-clinic practices toward cloud-native PACS with elastic storage scaling.
Cloud-based ophthalmology PACS provides a centralized archive accessible across all practice locations. Floating clinicians and rotating subspecialists access patient imaging from any clinic without VPN or manual file transfer. Referring-specialist workflows — general ophthalmology to retinal, glaucoma, or oculoplastic subspecialists — happen in seconds rather than days. Multi-clinic practice management integration surfaces imaging in the patient chart across the network.
Cloud-based ophthalmology PACS typically runs $300-$1,000 per clinic per month for small single-clinic deployments, with enterprise pricing for multi-site ophthalmology groups. On-premise deployments have higher upfront costs ($10,000-$40,000 in hardware, software, and integration) with lower ongoing fees but operational IT overhead. OCT-heavy practices typically pay a storage premium across both deployment models, given the file size characteristics of OCT volumes.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo