From Manual to AI: The Future of Cardiac MRI Segmentation

What if a heart scan could reveal life-saving details in the time it takes to sip your coffee? That’s the promise of modern cardiac MRI segmentation.
Cardiac MRI segmentation is the process of dividing scans into the left ventricle, right ventricle, and myocardium. These boundaries help doctors to measure volumes, calculate ejection fraction, and detect heart disease with precision.
Let’s explore how segmentation works, why automation matters, and how deep learning is reshaping the future of cardiac imaging.

What Is Cardiac MRI Segmentation?
Cardiac MRI segmentation involves training a computer to identify and “draw boundaries” around the heart’s key components in an MRI scan. Instead of looking at a gray, complex image, segmentation divides the scan into three main regions:
- Left ventricle (LV): the heart’s main pumping chamber that sends oxygen-rich blood to the body.
- Right ventricle (RV): the chamber that pumps blood to the lungs for oxygenation.
- Myocardium: the muscular wall of the heart that contracts and relaxes with every beat.
By separating these areas, segmentation transforms raw MRI data into structured information that can be measured and analyzed.
Why Segmentation Matters in Cardiac MRI?
Segmentation is the foundation of cardiac measurement. Once the LV, RV, and myocardium are identified, doctors can calculate:
- End-diastolic volume (EDV): how much blood fills the ventricles before contraction.
- End-systolic volume (ESV): how much blood remains after contraction.
- Ejection fraction (EF): the percentage of blood pumped out with each beat — a vital marker for heart health.
These numbers are central to diagnosing heart failure, hypertrophic cardiomyopathy, dilated cardiomyopathy, and congenital defects. They guide decisions on whether a patient needs medication, surgery, or devices like pacemakers and defibrillators.
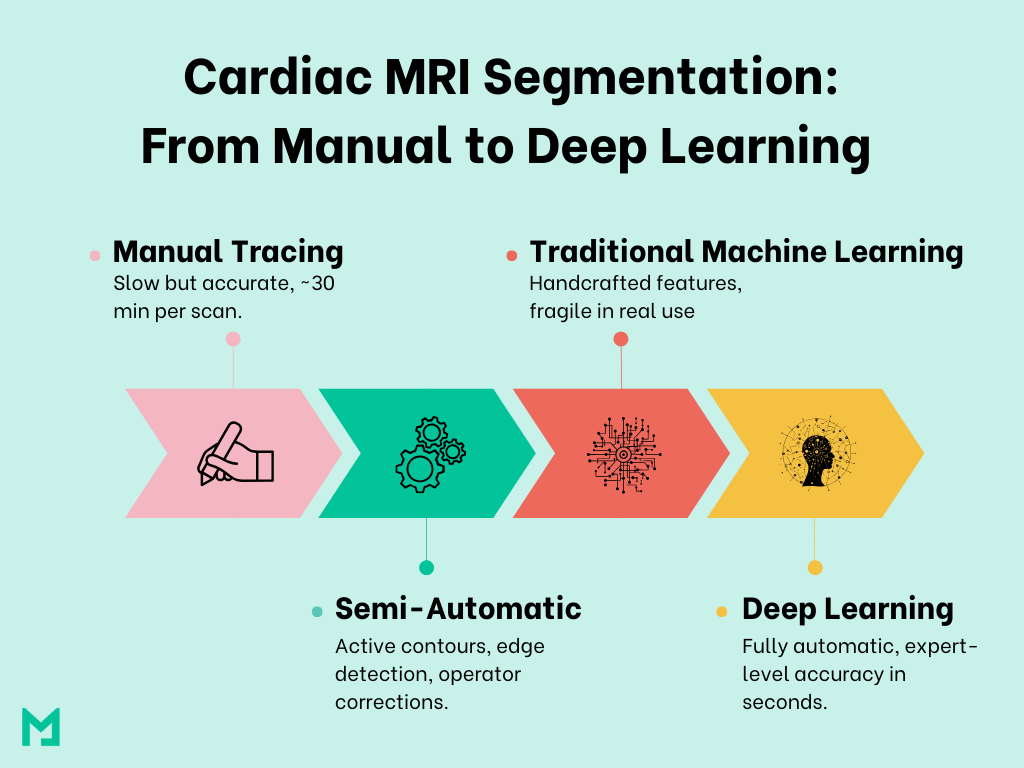
The Shift Toward Automation
Cardiac MRI segmentation used to be a manual, tedious process requiring radiologists to trace heart chamber boundaries on each scan slice. However, advancements in computer vision and AI have automated this process, significantly improving speed and reliability.
Manual Methods
In manual segmentation, every contour of the left ventricle, right ventricle, and myocardium is drawn by hand across dozens of MRI slices and time frames. A single patient’s dataset can involve hundreds of images, requiring 20–30 minutes of work per scan.
While the results are accurate, the process is exhausting, prone to fatigue, and impractical in high-volume clinical settings.
Semi-Automatic Methods
To reduce the burden, semi-automatic tools like active contour models and edge-detection algorithms were introduced. These methods could outline structures automatically, but they were highly dependent on image quality and still required manual correction.
For example, poor contrast at the apex or basal slices often confused the algorithms, forcing radiologists to step in and adjust. The result: some time saved, but workflows are still slow and inconsistent.
Traditional Machine Learning
Traditional machine learning methods marked the next stage. Instead of simple rules, they used handcrafted features (like texture or intensity) to detect chamber boundaries. These algorithms performed better than basic edge detectors but were fragile in real-world use.
A model trained on one dataset often failed on another due to variations in scanners, patient anatomy, or artifacts. Clinical reliability remained out of reach.
The Deep Learning Revolution
The real breakthrough came with deep learning, particularly convolutional neural networks (CNNs). Unlike traditional methods, CNNs learn directly from vast datasets of annotated MRIs, extracting both global heart shapes and fine structural details.
The U-Net architecture, with its encoder–decoder design and skip connections, became the backbone of cardiac MRI segmentation. U-Net and its many improved variants (residual U-Net, attention U-Net, 3D U-Net) demonstrated expert-level accuracy in seconds.

Deep Learning Models Driving Progress
Deep learning has turned cardiac MRI segmentation from an academic challenge into a clinical reality, achieving human-expert level accuracy in less time by learning from extensive imaging data.
U-Net: The Backbone of Cardiac Segmentation
The U-Net model is the foundation of most modern cardiac segmentation tools. Its design includes:
- Encoder path: compresses the input image into high-level features (shapes, textures).
- Decoder path: reconstructs the image, labeling each pixel as LV, RV, myocardium, or background.
- Skip connections: link the encoder and decoder, preserving fine details so chamber walls aren’t lost in the process.
The U-Net’s structure is ideal for medical images, providing both global understanding and pixel-level accuracy.
Smarter Variants and Improvements
While the U-Net provided the breakthrough, researchers soon developed enhanced versions to boost accuracy.
- Residual U-Nets: improve training stability and allow deeper networks.
- Attention U-Nets: help the model “focus” on chamber borders while ignoring noise.
- 3D U-Nets: process entire volumes of slices, ensuring smoother segmentation across the heart’s short-axis stack.
- PrimUNet: a novel design which achieved Dice ≈0.91 for LV/RV and 0.89 for myocardium in real-time MRI of non-human primates
These improvements make deep learning powerful even in challenging cases like arrhythmia, congenital defects, or poor image quality.
Accuracy Benchmarks Across Studies
The strength of deep learning lies in its results.
In a large evaluation of human cine MRI scans, deep learning achieved outstanding accuracy. The reported Dice scores were 0.965 for LV, 0.929 for RV, and 0.909 for the myocardium.
Reports also show high Dice scores, usually over 0.90 for LV segmentation, with very good scores for RV and myocardium in cine MRI scans using deep learning models.
In a deep learning evaluation for cine CMR segmentation, Dice coefficients exceeded 0.95 for LV and 0.90 for myocardium and RV.
The results show that AI-driven segmentation accurately measures chamber volumes and myocardial thickness, demonstrating its reliability in real-world clinical use.
Real-Time MRI: A New Frontier
One of the most exciting developments is the extension of segmentation into real-time MRI. Unlike cine MRI, which requires multiple breath-holds and longer acquisition times, real-time MRI captures the heart continuously.
Deep learning models can now segment these frames beat-by-beat, enabling:
- Strain analysis: measuring how myocardial fibers stretch and contract each beat.
- Arrhythmia studies: analyzing patients with irregular rhythms where cycle lengths vary.
- Preclinical applications: shown in non-human primates, proving that models can bridge research and clinical domains.
This expansion shows that segmentation is now more than just a tool for post-processing. It is becoming a real-time tool that can be used in clinical settings.

Evaluation Metrics That Matter
AI models in medicine, such as cardiac MRI segmentation, require robust metrics to establish trust. Employing various metrics guarantees that models are not only mathematically sound but also clinically reliable.
Dice Similarity Coefficient (DSC)
The Dice score measures how much the automated segmentation overlaps with expert-drawn ground truth. A score close to 1.0 means near-perfect alignment. For cardiac MRI, Dice values above 0.9 are considered excellent and clinically reliable.
Hausdorff Distance (HD)
The Hausdorff distance looks at the worst-case boundary errors. Even if most of the segmentation is accurate, large outliers in boundaries can impact clinical use. Lower HD means the model is capturing contours more precisely.
Average Symmetric Surface Distance (ASSD)
ASSD measures the average distance between the segmented boundary and the ground truth. This smooths out variability and provides a balanced view of accuracy across the entire heart structure.
Clinical and Research Applications
Beyond raw numbers, the true value of cardiac MRI segmentation lies in its impact on patients and research. Automatic, accurate segmentation opens doors to faster diagnoses, smarter treatment planning, and even breakthroughs in translational science.
Quantifying Cardiac Function
Segmented LV and RV boundaries allow precise calculation of end-diastolic volume (EDV), end-systolic volume (ESV), and ejection fraction (EF). These measurements are critical for assessing heart performance and detecting early signs of heart failure or cardiomyopathy.
Myocardial Strain Analysis
In real-time MRI, segmentation enables beat-to-beat analysis of myocardial strain: how the heart muscle stretches and contracts. It provides a deeper view of heart mechanics and can guide interventions before structural damage becomes visible.
Disease Monitoring and Prognosis
Consistent segmentation across timepoints helps clinicians to track disease progression, measure therapy response, and adjust treatments with confidence. From hypertrophic cardiomyopathy to dilated ventricles, chamber volumes tell the story of disease trajectory.
Preclinical and Translational Research
Studies in non-human primates (NHPs) have shown that deep learning models can segment real-time MRI with Dice scores around 0.9, mirroring human performance. This strengthens the bridge between lab research and clinical practice.
Key Challenges and Future Directions
Deep learning has made cardiac MRI segmentation fast and accurate, but there are still some challenges to solve before it can be used everywhere in daily clinical practice.
Difficult Chamber Boundaries
The apex of the heart and the valve plane are challenging areas, and even top models can struggle to mark them accurately. Small errors can significantly impact metrics like ejection fraction.
Researchers are exploring new methods, including attention U-Nets, to improve handling of these regions.
Scar and Fibrosis Segmentation
While chambers are segmented well, detecting scar tissue or fibrosis in the myocardium is still a challenge. In many studies, Dice scores for scar segmentation are much lower (often below 0.8). This matters because scar burden is key to managing heart failure and arrhythmia patients.
Generalizability Across Scanners and Populations
A significant issue is that models trained in one hospital may not perform as well in another. Differences in MRI scanners, settings, and patient groups affect performance.
Data Limitations
Deep learning needs large, diverse datasets. But in medicine, data is often limited because annotations take so much expert time. New approaches like federated learning (training models across hospitals without sharing raw data) may help solve this issue.
Future Direction of Cardiac MRI Segmentation
Future research is focusing on:
- Better architectures that combine CNNs with transformers or hybrid models for improved precision.
- Explainable AI, so doctors can understand why a model made a decision.
- Integration into PACS and hospital systems, so segmentation happens automatically in the background during scans.
- Multi-modal imaging, where MRI segmentation is combined with CT or echocardiography data for a full picture of heart health.
Conclusion
Cardiac MRI segmentation has moved from slow manual tracing to fully automatic AI tools that deliver expert-level accuracy in seconds. By ensuring speed, consistency, and reproducibility, deep learning is reshaping how doctors diagnose and monitor heart disease.
With solutions like Medicai, hospitals can integrate automation directly into their workflows, giving clinicians faster insights and patients more personalized care.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo