Radiology Information System (RIS): Modules, Chain Position, KPIs, and How It Connects HIS and PACS

RIS is the administrative and operational nervous system of a radiology department. It manages every event in the patient’s radiology journey, excluding the image itself — the referral, scheduling, patient check-in, exam tracking, report distribution, billing, and department statistics.
While PACS manages pixel data (the images), and HIS manages enterprise patient identity (the record), RIS manages the radiology workflow state—the sequence of status transitions from “order received” to “report distributed and billed” — that occurs between those two systems.

| System | Scope | Primary data type | What does it know about the patient |
| HIS | Enterprise — whole hospital | Administrative, clinical, and financial | Everything — master patient identity, all encounters, all orders across all departments |
| RIS | Departmental — radiology only | Administrative + workflow state | Patient demographics (received from HIS), radiology orders, exam status, radiology reports, radiology billing |
| PACS | Departmental — imaging archive | DICOM image data | Study-level data (accession number, modality, series), image metadata — depends on RIS for order context |
| EHR/EMR | Clinical — patient medical record | Clinical documentation | Clinical history, diagnoses, medications — receives radiology reports from RIS via ORU |
The six functional modules of the Radiology Information System (RIS)
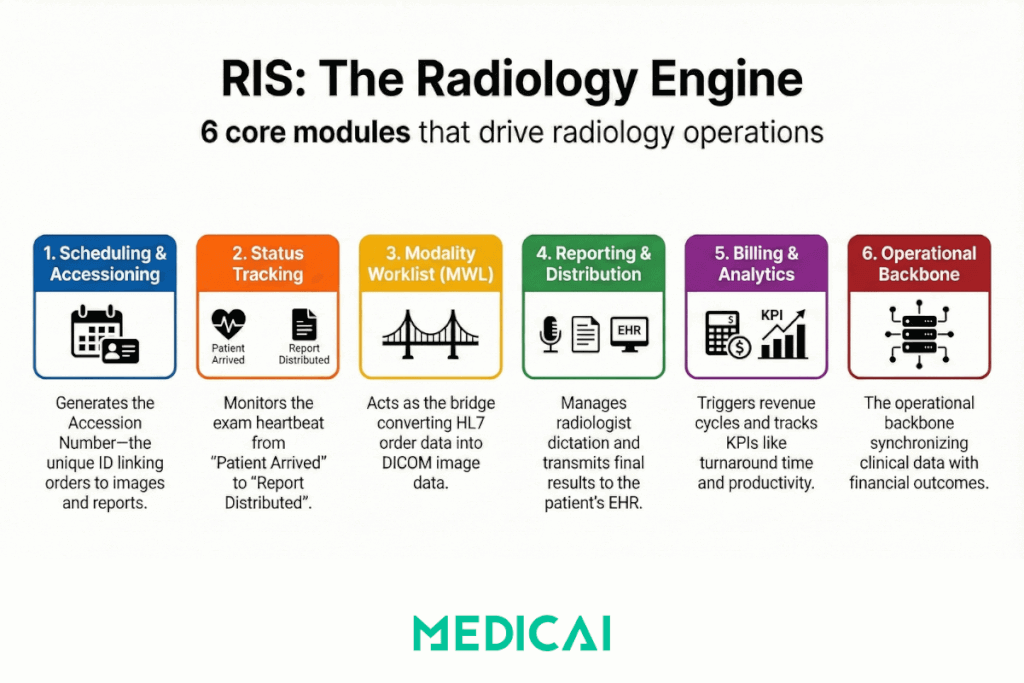
Module 1 — Patient scheduling and appointment management
This is what most people mean when they say “RIS.” The scheduling module receives the imaging order (from HIS via HL7 ORM, or directly from CPOE in integrated systems), checks resource availability (modality, room, radiologist), assigns an appointment slot, and generates the accession number.
The accession number is the most consequential act the scheduling module performs — it is the unique identifier that ties the imaging order to the image file, the radiology report, and the billing record. If the accession number is malformed, duplicated, or absent, the entire downstream chain breaks. The scheduling module is also where patient demographics are first confirmed in the RIS — the moment where a mismatch between HIS identity and the scheduled exam becomes visible, or doesn’t.
Module 2 — Exam tracking and status management
Once the appointment is scheduled, RIS tracks the exam through its lifecycle states: Scheduled → Patient Arrived → In Progress → Exam Complete → Report Pending → Report Signed → Report Distributed. This status chain is the operational heartbeat of the radiology department. Every downstream event, worklist visibility, billing trigger, and result notification to the referring physician depends on status transitions happening correctly and on time.
The workflow manager in PACS reads exam status from RIS to route studies to the right reading queue. When exam status transitions fail silently (a common interface-engine failure mode), studies become invisible to the workflow manager even though they are present in the PACS archive.
Module 3 — Modality Worklist Server
The RIS acts as the Modality Worklist (MWL) server — the system that responds to DICOM C-FIND queries from imaging devices. When a technologist activates a patient study at the CT scanner, the scanner sends a C-FIND query to the RIS’s MWL server. The RIS responds with the scheduled examination details: patient demographics, accession number, procedure code, and ordering physician.
This is the moment where HIS-originated order data becomes DICOM data — the modality pre-populates its DICOM tags from the MWL response, ensuring that the image file arriving at PACS carries the same identifiers as the RIS order. The MWL server is the junction point between the HL7 world (HIS and RIS) and the DICOM world (modality and PACS).
Module 4 — Radiology reporting module
After the exam is complete and the images are in PACS, the radiologist reads the study and dictates the report. The reporting module manages the report lifecycle: report creation (via dictation system, voice recognition, or structured reporting tool), transcription or direct entry, radiologist signature (attestation), and report distribution. Distribution means sending the signed report back to HIS via an HL7 ORU message for storage in the patient’s EHR and making the report available to the referring physician through the institution’s access channel.
The reporting module is where structured reporting integrates with RIS — the structured report template lives in a reporting tool. Still, the signed report is transmitted and stored through RIS’s distribution infrastructure. The ORU message failure mode (report finalized in RIS but never received by HIS) is the most consequential single-point failure in the result return chain.
Module 5 — Billing and revenue cycle management
When the report is signed, RIS triggers the billing workflow. The billing module links the performed procedure (CPT code) to the diagnosis codes from the report (ICD-10), generates the charge, and transmits the claim to the hospital’s billing system or directly to the payer. RIS is the source of truth for radiology billing — it knows what was ordered, what was performed, what the radiologist found, and what codes attach to that finding.
Billing module failures are often invisible to the clinical team but financially significant: an ORU transmission failure that prevents report finalization also prevents the billing trigger, causing silent underbilling. A procedure code mismatch between the HIS order and the RIS schedule results in claim denials that take weeks to surface.
Module 6 — Statistics, QA, and reporting analytics
The statistics module aggregates exam volume, report turnaround time, radiologist productivity (RVUs), equipment utilization, and cancellation rates. This is the data layer that department leadership uses to manage capacity and identify workflow bottlenecks. It is also the source for regulatory reporting and accreditation documentation. The statistics module is where RIS KPIs become visible, which leads naturally into the next section.
Radiology Information System KPIs — how radiology departments measure RIS performance
Report Turnaround Time (TAT)
Time from exam completion to signed report distribution. Measured separately for emergency (target: under 1 hour for stat reads), urgent (target: under 4 hours), and routine studies (target: under 24 hours). TAT is the single most important operational KPI in radiology — it determines clinical utility of the imaging result and is a direct quality indicator for accreditation bodies, including ACR and The Joint Commission. RIS is the system of record for TAT measurement because it captures both the exam completion timestamp and the report distribution timestamp.
Scheduling Fill Rate
Percentage of available appointment slots that are filled within a defined window. Target varies by modality and institution (typically 85-95% for high-demand modalities). A low fill rate indicates either excess capacity or scheduling friction — orders being placed but not converting to appointments, often due to insurance pre-authorization failures or patient no-shows that aren’t being backfilled.
Unread Study Queue Depth
Number of studies in PACS that have been acquired but not yet read. This is a downstream measure of RIS scheduling and workflow efficiency — a deep unread queue indicates either volume exceeding reading capacity or workflow manager routing failures that leave studies unassigned. RIS tracks unread studies via its status module; PACS displays the queue. When they disagree, a status synchronization failure occurs between RIS and PACS.
Exam Cancellation and No-Show Rate
Percentage of scheduled exams that are cancelled before completion. Target is typically below 10% for elective scheduling. High cancellation rates consume capacity and indicate scheduling quality problems — exams being scheduled before clinical prerequisites (pre-authorization, patient preparation instructions, contrast allergy screening) are confirmed.
Modality Utilization Rate
Percentage of available scanner time that is in productive use. Calculated from exam duration data in RIS against scheduled hours. Underutilization is a capital efficiency problem; overutilization creates access delays and deferred maintenance. RIS scheduling data is the input for modality utilization reporting.
ORU Transmission Success Rate
Percentage of signed reports successfully transmitted to HIS/EHR via HL7 ORU. Target: 99.9% or higher. Any failure rate above 0.1% creates both clinical risk (the referring physician doesn’t receive the result) and financial risk (the billing trigger doesn’t fire). This KPI bridges RIS performance to HIS integration quality — most ORU failures originate in interface engine configuration or HIS-side message handling, not in RIS itself.
RIS position in the HIS to RIS to PACS chain
A table mirroring the format from the HIS blog’s event chain table, but from RIS’s perspective — what RIS receives, what it does with it, what it sends downstream.
| Upstream event (from HIS) | What RIS does | Downstream effect (in PACS/modality) |
| ADT A01 — patient admission | RIS creates or updates the patient record with demographics from HIS MPI. First opportunity for identity mismatch if HIS data is malformed. | PACS receives patient identity via subsequent ORM. If A01 demographics are incorrect, all downstream image files contain incorrect metadata. |
| ORM O01 — imaging order | RIS creates a scheduled examination. Assigns accession number. Makes the exam visible to the scheduling module. | The Modality Worklist server becomes queryable for this exam. Without ORM, there is no worklist entry, and the technologist must manually enter data — primary source of transcription errors in PACS. |
| ADT A08 — patient demographic update | RIS updates the patient record. Late-arriving A08 messages indicate that the scheduled exam contains outdated demographics. | If A08 arrives after the MWL query has already been executed at the modality, the scanner already pre-populated DICOM tags with the old name. The PACS study carries the wrong demographics. |
| ADT A40 — patient merge | RIS must reconcile all historical scheduled and completed exams for the merged patient. Most operationally complex ADT event in RIS. | If RIS does not propagate the merge to PACS (via a matching A40 transaction or equivalent), PACS retains split patient history — studies from different MRNs that belong to the same patient remain separated. |
| No event — order cancelled in HIS without a cancel message | RIS retains the scheduled exam on the worklist. A technologist may perform an exam that has been clinically cancelled. | PACS acquires and archives a study that has no valid order in the HIS. Billing cannot process a claim without a matching order. |
And the reverse direction — what RIS sends upstream and downstream:
| RIS event | Upstream effect (in HIS) | Downstream effect (in PACS/modality) |
| Accession number assigned | None directly — accession number is RIS-generated | Modality pre-populates DICOM tags with the accession number. PACS uses an accession number to link the image file to the order. |
| Exam status → Complete | None directly | PACS workflow manager moves the study from “acquired” to the “ready for reading” queue. |
| ORU R01 — report signed | HIS receives report, stores in EHR, notifies referring physician, triggers billing | None — report return is HIS-bound |
| MWL query response (DICOM C-FIND) | None — MWL is modality-facing | Modality pre-populates DICOM tags. This is the junction where HL7 order data becomes DICOM metadata. |
Radiology Information System challenges
Vendor fragmentation and integration maintenance cost
Most hospital radiology departments have RIS and PACS systems from different vendors, connected through an interface engine. Every RIS upgrade is a potential interface regression — HL7 message format changes in the new RIS version may break the ORM parsing logic in the interface engine, causing silent worklist failures. Interface engine maintenance is an ongoing operational cost that most IT departments underestimate at the time of procurement.
Legacy data migration when replacing RIS
Historical exam records, accession numbers, and report archives stored in a legacy RIS must be migrated to the new system without breaking the links between order records and PACS images. Accession number continuity is the core risk — if the new RIS generates accession numbers in a different format than the old system used, pre-migration studies in PACS become orphaned from any order record in the new RIS. This makes prior study retrieval unreliable for any exam that predates the migration.
Incomplete CPOE adoption and workaround management
When clinicians place orders outside the formal CPOE workflow — verbal orders, paper requisitions, direct calls to the radiology department — RIS receives no ORM message from HIS. The scheduling module must create the exam record manually, with no HIS-originated accession number assignment, no automatic demographics population, and no billing pre-authorization trigger. Manual order entry is the single largest source of accession number errors and unmatched studies in PACS for institutions that have not fully implemented CPOE.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo