Teleradiology Services: Cost, Workflow, and What to Look for in a Provider

Teleradiology services are remote radiological interpretation offerings provided by radiology groups, hospital networks, and dedicated teleradiology companies to healthcare facilities that lack on-site radiologist coverage during specific hours, in specific subspecialties, or at specific volumes. The service includes the radiologist’s professional interpretation, the structured diagnostic report delivered to the ordering physician, and the technical infrastructure that transmits the imaging study from the originating facility to the interpreting radiologist.
The US teleradiology services market is mature and consolidated, with major providers including vRad (Virtual Radiologic, owned by RadPartners), Statrad, Consulting Radiologists, ProScan, RAYUS Radiology, and National Diagnostic Imaging operating large remote reading panels. The market also includes dozens of regional and subspecialty-focused teleradiology groups serving specific geographic or clinical niches. For a healthcare administrator evaluating teleradiology services, the decision is rarely whether to use teleradiology — most US hospitals already use it for at least some portion of their imaging interpretation workflow. The decision is which provider, what scope of coverage, what pricing model, and what technical integration approach. This guide covers each of those decisions in operational detail.
Types of Teleradiology Services Available
Teleradiology services fall into five primary categories distinguished by coverage scope and service model. A practice typically uses more than one — for example, after-hours coverage from one provider and subspecialty consultation from another.
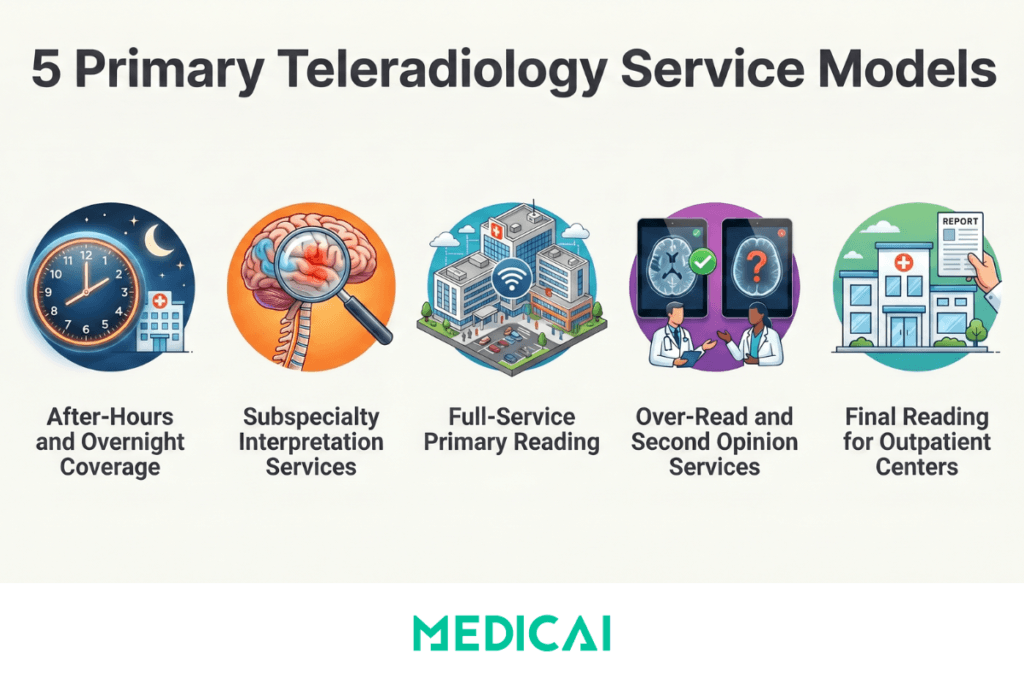
1. After-hours and overnight coverage (Nighthawk Teleradiology)
The most common teleradiology service model. The provider covers imaging interpretation during hours when in-house radiologists are not available — typically overnight, weekends, and public holidays. Studies are routed to the teleradiology panel as they are acquired, interpreted within the agreed turnaround time (typically 30 minutes for emergency studies, 1-4 hours for routine after-hours studies), and the structured report is delivered to the ordering physician’s EHR. The in-house radiology team resumes interpretation responsibility during standard business hours.
2. Subspecialty interpretation services
Used when the originating facility lacks subspecialist coverage in specific clinical areas. Common subspecialty teleradiology services include pediatric radiology, neuroradiology, musculoskeletal radiology, breast imaging, nuclear medicine, and cardiac imaging. Studies in the relevant subspecialty are routed to the subspecialist teleradiologist rather than the general teleradiology panel. Subspecialty teleradiology typically carries premium per-study pricing reflecting the specialized expertise required.
3. Full-service teleradiology (primary reading)
The teleradiology service provides all imaging interpretation for the originating facility — replacing rather than supplementing in-house radiologists. Used by small clinics, urgent care networks, and imaging centers that cannot justify in-house radiologist staffing economically. Full-service teleradiology typically includes 24/7 coverage, subspecialty access, and quality assurance review built into the contract.
4. Over-read and second opinion services
Teleradiology provides a second radiologist’s interpretation of a study already read by the originating facility’s radiologist. Used for quality assurance programs, second opinions on complex cases, and in some clinical settings (urgent care, emergency departments) where physician assistants or nurse practitioners perform an initial preliminary read and a teleradiologist provides the official signed report. The over-read service has specific billing and medico-legal considerations distinct from primary reading.
5. Final reading services for outpatient imaging centers
Used by imaging centers without their own radiology group affiliation. The teleradiology service reads all outpatient imaging studies, delivers reports to ordering physicians, and bills the professional component of the imaging service to the patient’s insurance. The imaging center operates the imaging equipment and bills the technical component; the teleradiology service handles the interpretation and professional billing.
Teleradiology Service Costs and Pricing Models
Teleradiology pricing is structured under three primary models: per-study, per-shift, and full-service contract. Each fits a different practice scenario, and the right model depends on study volume, coverage scope, and the predictability of the practice’s imaging demand.
Per-study pricing — typical range and what it covers
Per-study pricing is the most common model for after-hours and overnight teleradiology coverage. Typical pricing in the US market ranges from $15 to $45 per study, with the specific rate depending on study type (X-ray cheapest, complex MRI most expensive), turnaround time requirements (faster TAT carries premium pricing), subspecialty requirements (subspecialty interpretation costs more than general radiology), and contract volume (high-volume contracts negotiate lower per-study rates). For a community hospital with 200 after-hours studies per month, per-study pricing typically produces a monthly cost of $4,000 to $9,000 — significantly less than the cost of in-house overnight radiologist coverage.
Per-shift pricing — fixed cost coverage
Per-shift pricing covers a defined block of teleradiology coverage (typically 8-hour or 12-hour shifts) at a fixed rate regardless of study volume during the shift. Typical rates range from $1,500 to $4,000 per shift, depending on subspecialty mix and SLA requirements. Per-shift pricing is preferred by practices with predictable high study volumes during coverage windows — at 100+ studies per shift, the effective per-study cost under shift pricing drops below typical per-study rates.
Full-service contract pricing
Full-service teleradiology contracts cover all the originating facility’s imaging interpretation at a negotiated monthly or annual rate. Contract structures vary widely — some include all clinical professional fees in the contract value, others bill the professional component to the insurance and add a smaller per-study or per-month fee to the facility. Annual full-service contracts for a small imaging center typically range from $200,000 to $800,000, depending on volume and subspecialty mix.
Cost comparison: teleradiology vs in-house radiology coverage
The economic case for teleradiology over in-house coverage is most clear for after-hours and subspecialty coverage. A full-time radiologist costs $400,000 to $650,000 per year in loaded compensation (salary, benefits, malpractice, licensing). For a small community hospital with 300 after-hours studies per month, teleradiology at per-study pricing produces an annual cost of approximately $54,000 to $162,000 — between 12% and 40% of the in-house cost. For practices with total monthly volume below approximately 4,000 studies, teleradiology is typically the only economically viable option. For higher-volume practices, the calculation includes in-house radiologist quality of life, retention, and burnout considerations — see the cloud PACS total cost of ownership framework for the full financial comparison.
How Teleradiology Service Workflows Operate
A teleradiology service workflow follows a six-step process from study acquisition to report delivery. Each step has specific technical and operational requirements that determine which service providers and which infrastructure platforms can support which workflows.
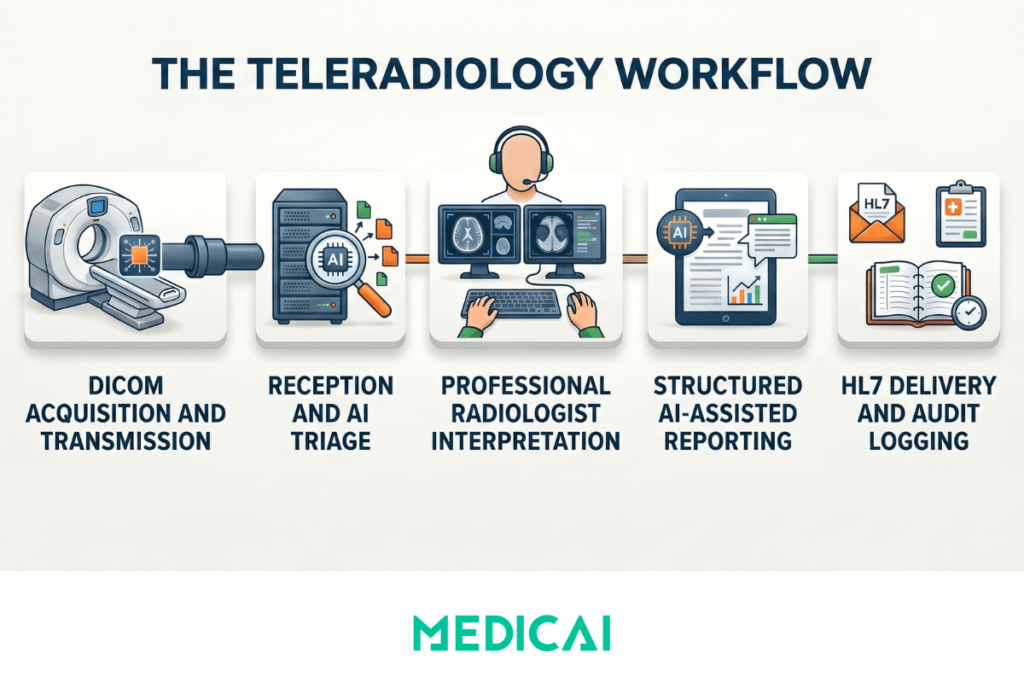
- Step 1 — Study acquisition and DICOM transmission. The imaging modality (CT, MRI, X-ray, ultrasound) at the originating facility acquires the study and transmits it via DICOM to the teleradiology service. Transmission occurs either through a DICOM Gateway at the originating site (which forwards studies to a cloud archive over HTTPS) or through direct DICOM connection to the teleradiology service’s on-premise or cloud archive. The Gateway approach is increasingly standard because it does not require VPN configuration or static IP addressing at the originating site.
- Step 2 — Study reception and worklist placement. The teleradiology service’s central platform receives the DICOM study, validates that all required series are present, and places it on the appropriate radiologist’s reading worklist based on study type, subspecialty, urgency, and the radiologists available on the panel. AI triage tools (Viz.ai for stroke, Aidoc for multi-pathology, similar products) may operate at this step to flag suspected critical findings and reorder the worklist before the radiologist opens any study.
- Step 3 — Radiologist interpretation. The teleradiologist opens the study in a diagnostic DICOM viewer — typically a zero-footprint browser-based viewer for cloud-native services, or a thick-client viewer for legacy on-premise systems. The radiologist reviews the study, compares it with prior studies if available, and interprets the imaging findings. Diagnostic display calibration and reading environment quality (lighting, monitor specification) are the radiologist’s professional responsibility and a critical quality factor in teleradiology — addressed through the ACR Technical Standard for Teleradiology and equivalent practice standards.
- Step 4 — Structured report generation. The radiologist generates the diagnostic report — typically using AI-assisted dictation and structured reporting templates that produce a consistent report format. AI tools at this step may include speech recognition optimized for radiology vocabulary (Nuance PowerScribe), NLP-based template population, and AI-drafted impression sections. The completed report is signed by the radiologist with an electronic signature.
- Step 5 — Report delivery via HL7. The structured report is delivered to the ordering physician’s EHR via an HL7 ORU message, populating the imaging report field in the patient’s record. Critical findings (acute hemorrhage, large-vessel occlusion stroke, pneumothorax) typically trigger additional notification workflows — such as a direct phone call to the ordering physician, secure messaging, or critical results notification systems built into the teleradiology platform.
- Step 6 — Quality assurance and audit logging. The teleradiology service maintains audit logs of every study, including access, interpretation, and report delivery, for clinical quality assurance, medico-legal documentation, and HIPAA compliance. Many services also operate prospective peer review programs — a percentage of studies are re-read by a second radiologist to monitor diagnostic accuracy and identify cases requiring clinical correlation or follow-up.
How to Evaluate Teleradiology Service Providers: 10 Criteria
Ten criteria for evaluating teleradiology service providers, ordered by the typical buyer evaluation sequence. Use this as a structured framework for comparing providers — every criterion should produce a documented answer before a contract is signed.
| # | Evaluation criterion | What to verify before signing the contract |
|---|---|---|
| 1 | Coverage scope and Service Level Agreement | What hours are covered (after-hours only, weekends, holidays, 24/7)? What turnaround time is guaranteed for STAT, urgent, and routine studies? What is the contractual remedy if the SLA is missed — credit, service extension, or partial refund? |
| 2 | Subspecialty coverage | Which subspecialties are available — paediatric radiology, neuroradiology, musculoskeletal, breast imaging, nuclear medicine, cardiac imaging? What is the rate-card differential for subspecialty studies vs general radiology interpretation? |
| 3 | Radiologist credentials and licensure | Are all radiologists US-trained and board-certified by the American Board of Radiology or equivalent? In which states are they licensed? How is licensure verified and maintained for radiologists reading studies from patients in the practice’s state? |
| 4 | Quality assurance programme | What percentage of studies receive peer review or double-read for quality assurance? How are discrepancies flagged, communicated to the originating facility, and resolved? What is the documented diagnostic accuracy rate and how is it measured? |
| 5 | Technical integration capabilities | Does the service integrate with the originating site’s PACS via DICOM Gateway (preferred) or DICOM C-STORE? With the RIS via HL7 ORM and ORU messages? With the EHR via HL7 or FHIR DiagnosticReport? What one-time integration costs and ongoing interface maintenance fees apply? |
| 6 | Pricing model and total expected cost | What is the pricing model — per-study ($15–$45 typical), per-shift ($1,500–$4,000 typical), or full-service contract ($200,000–$800,000 annual)? What is the total expected annual cost at projected study volume? What add-on fees apply for after-hours, STAT studies, or subspecialty interpretation? |
| 7 | HIPAA compliance and data security | Is a signed HIPAA Business Associate Agreement provided as a standard contract term? What encryption standards apply (AES-256 at rest, TLS 1.2+ in transit)? What is the breach notification protocol and contractual notification window? |
| 8 | Reporting standards and customisation | Are structured reports delivered in the originating facility’s preferred format (free-text, structured, RSNA RadReport templates)? Can templates be customised per ordering physician or per study type? Are critical results notification protocols configurable for direct physician contact? |
| 9 | AI tool integration | Does the service operate AI triage tools (Viz.ai for stroke, Aidoc for multi-pathology, RapidAI for PE) for critical finding prioritisation? Are CAD AI overlays delivered with the study to the radiologist? Are AI-assisted dictation and structured reporting tools deployed? |
| 10 | Contract terms and data portability at exit | What is the contract length and renewal structure (auto-renewal vs negotiated)? What notice period is required for termination? What is the data export process, format (DICOM with full metadata), per-study export fee, and maximum time to complete a full archive export at contract end? |
Major US Teleradiology Service Providers
The US teleradiology services market includes both large national providers and regional or subspecialty-focused groups. The named providers below are illustrative of the market structure — buyers should evaluate each provider against the criteria framework above rather than selecting based on brand recognition alone.
National providers operating large reading panels include vRad (Virtual Radiologic, owned by RadPartners), Statrad, Consulting Radiologists, ProScan, RAYUS Radiology, and National Diagnostic Imaging. These providers typically offer 24/7 coverage, subspecialty access, and multi-state licensure spanning most US states. National provider contracts are typically larger in scope and include integration and onboarding professional services as part of the contract value.
Regional teleradiology groups operate on a smaller scale, often serving a specific multi-state region or clinical specialty. Regional providers may offer competitive pricing for smaller-volume contracts and more flexible service customization than national providers can typically support. The regional provider market includes dozens of groups across the US. Local hospital networks and specialty societies often maintain referral lists of regional teleradiology providers serving their geographic area.
Subspecialty-focused teleradiology services serve specific clinical specialties — pediatric radiology (NightHawk Pediatric Radiology, Children’s Healthcare of Atlanta Teleradiology), neuroradiology, breast imaging, and nuclear medicine. Subspecialty providers typically command premium per-study pricing and operate at smaller volumes than general teleradiology services.
Where Medicai fits
Medicai is not a teleradiology service provider — Medicai does not employ radiologists or operate a reading panel. Medicai is the cloud PACS infrastructure layer that teleradiology services, hospital networks, and imaging centers use to operate their teleradiology workflows. The DICOM Gateway, cloud archive, zero-footprint viewer, and HL7 integration described in the workflow section are teleradiology infrastructure components that Medicai provides. Healthcare administrators evaluating teleradiology services often also evaluate the underlying infrastructure — particularly when moving from on-premise PACS to cloud-native architecture as part of a teleradiology adoption decision.
Frequently Asked Questions
How much do teleradiology services cost?
Teleradiology services in the US typically charge $15 to $45 per study under per-study pricing, $1,500 to $4,000 per shift under per-shift pricing, or $200,000 to $800,000 annually under full-service contract pricing for a small imaging center. The specific cost depends on coverage scope (after-hours only versus full primary reading), subspecialty mix (subspecialty interpretation costs more than general radiology), turnaround time requirements (STAT studies carry premium pricing), and total contract volume (higher volumes negotiate lower per-study rates). For most community hospitals using teleradiology for after-hours coverage, the monthly cost ranges from $4,000 to $20,000, depending on the volume of studies.
Who are the major teleradiology service providers?
Major US teleradiology service providers include vRad (Virtual Radiologic, owned by RadPartners), Statrad, Consulting Radiologists, ProScan, RAYUS Radiology, and National Diagnostic Imaging at the national scale. Dozens of regional and subspecialty-focused teleradiology groups also operate in the US market, often serving specific geographic regions or clinical specialties such as pediatric radiology, neuroradiology, or breast imaging. The right provider depends on coverage scope, subspecialty requirements, and pricing model fit — there is no single best teleradiology provider for all use cases.
What is the difference between teleradiology services and teleradiology software?
Teleradiology services are radiology groups that provide remote interpretation as a professional service — they include radiologists who read the studies and produce diagnostic reports. Teleradiology software is the technology infrastructure that enables remote interpretation — cloud PACS, DICOM viewers, and worklist management platforms — but does not include the radiologists themselves. A healthcare facility may buy both: software to manage its imaging workflow, and a teleradiology service to provide interpretation coverage outside of in-house radiologist hours. Some providers offer both as bundled solutions; others specialize in either software (e.g., Medicai) or services.
How do teleradiology services integrate with our existing PACS?
Teleradiology services integrate with the originating facility’s PACS through standard DICOM protocols. The most common integration architecture uses a DICOM Gateway installed at the originating site that forwards studies to the teleradiology service’s archive over HTTPS — no VPN or static IP required. RIS integration typically uses HL7 ORM messages for worklist coordination and HL7 ORU messages for report delivery back to the originating facility’s RIS and EHR. Integration cost and complexity vary by service provider and by the technical compatibility of the originating site’s PACS and RIS — confirm the specific integration scope and any one-time professional services costs before signing the contract.
How fast is teleradiology turnaround?
Teleradiology turnaround time depends on the service tier and study urgency. STAT studies for suspected stroke, intracranial hemorrhage, or pulmonary embolism are typically interpreted within 30 minutes of arrival on the teleradiologist’s worklist, with critical findings communicated to the ordering physician within an additional 5 to 15 minutes. Urgent studies are typically interpreted within 1 hour. Routine after-hours studies are typically interpreted within 2 to 4 hours. The specific SLA is contractual and should be documented with measurable remedies for SLA breach. AI-assisted triage tools deployed within modern teleradiology services have reduced critical-finding time-to-notification by an average of 60% in emergency radiology settings.
Are teleradiology services HIPAA compliant?
HIPAA compliance is a baseline contractual requirement for any teleradiology service handling US patient data. Required elements include a signed HIPAA Business Associate Agreement from the teleradiology provider, AES-256 encryption of DICOM data at rest in the provider’s archive, TLS 1.2 or higher encryption for data in transit, role-based access controls restricting study access to credentialed radiologists, and complete audit logging of all study access events with timestamps and user identity. Teleradiology services operating across state lines must also verify radiologist licensure in each state where patient imaging occurs — the radiologist must be licensed in the patient’s state, regardless of the radiologist’s physical location.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo