PACS Interoperability, Standards, Benefits, Challenges, and Emerging Trends

A clinician opens a patient chart, clicks Imaging, and expects three things fast: the right study, the right priors, and a report that matches the images.
PACS interoperability determines whether that click results in a phone call, a screenshot, or a repeat scan. Interoperability connects modalities, PACS, RIS, EHRs, and downstream viewers so that images and context travel together. PACS interoperability protects workflow speed, patient identity integrity, and cross-site collaboration.
What is PACS interoperability, and what does it cover?
PACS interoperability is the ability of a PACS to exchange imaging data and clinical context with other healthcare systems without manual re-entry or format friction.
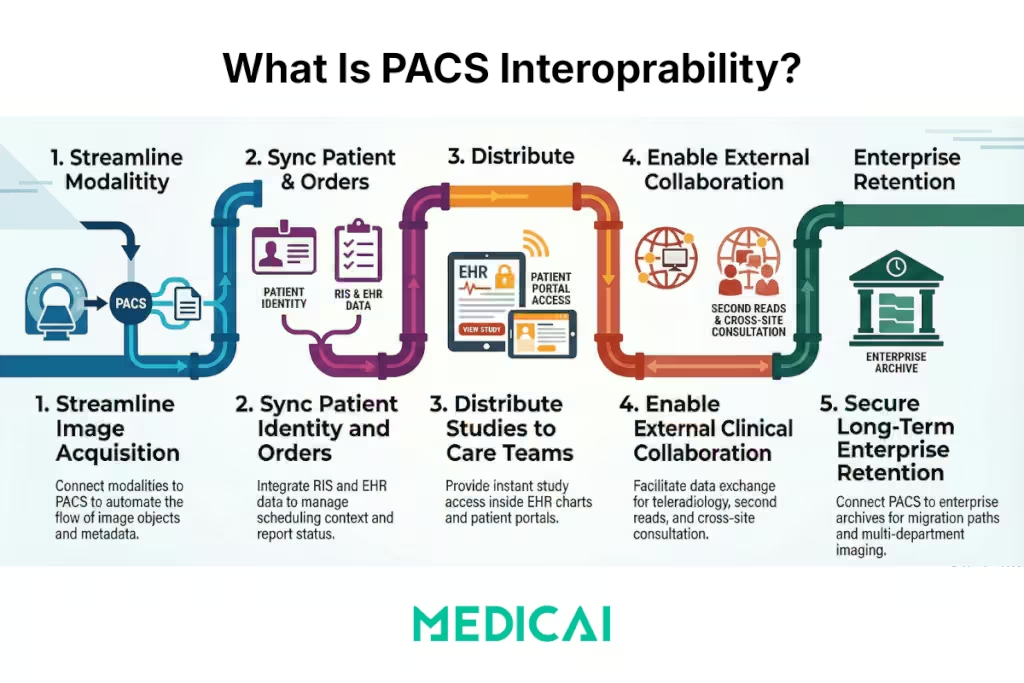
PACS interoperability scope covers five exchange paths.
- Modality to PACS, image objects, and acquisition metadata
- RIS and EHR to PACS, patient identity, orders, scheduling context, and report status
- PACS to EHR and portals, study access inside the chart, and distribution to care teams
- PACS to external readers, teleradiology, second reads, cross-site collaboration
- PACS to enterprise archives, long-term retention, migration paths, and multi-department imaging
PACS interoperability data types extend beyond pixels. It includes DICOM studies and series, patient and encounter identifiers, accession numbers, order context, report objects, and audit signals.
What are the four major components of PACS?
PACS interoperability depends on four components working in concert. Each plays a distinct role in the imaging chain, and interoperability breaks when any component operates in isolation from the others.
Component 1 — Imaging modalities
Modalities are the acquisition sources: CT, MRI, X-ray, ultrasound, PET, and others. Each modality generates DICOM objects and must be able to push those objects to the archive using DICOM Store. Interoperability starts at the modality level because a modality that cannot communicate study context to the PACS creates orphan acquisitions from the first step in the chain.
Component 2 — Archive and storage layer
The archive receives, indexes, and retains imaging objects. In traditional PACS, the archive is tightly coupled to the vendor’s viewer. In modern architectures, the archive is increasingly decoupled — either as a vendor-neutral archive (VNA) or a cloud object store — so that imaging objects can be retrieved by any authorized system, not just the originating PACS viewer. Interoperability depends on the archive exposing standard retrieval interfaces, primarily DICOM C-MOVE and WADO-RS, rather than proprietary access methods.
Component 3 — Viewing workstations and web viewers
Viewers consume images from the archive and display them to radiologists, clinicians, and referring providers. Interoperability at the viewer layer means the viewer can retrieve studies from any standards-compliant archive, launch within the EHR using FHIR context, and display studies regardless of originating vendor. Browser-based viewers using DICOMweb have significantly expanded interoperability at this layer by removing the requirement for a thick client installed on a specific workstation.
Component 4 — Network and communication infrastructure
The network layer moves imaging objects and clinical context between components. DICOM and HL7 messages rely on stable, low-latency connections. For multi-site deployments and teleradiology workflows, network performance directly determines whether priors arrive before the radiologist begins reading. VPN tunnels, dedicated DICOM routing appliances, and cloud-based DICOM brokers all operate at this layer.
For healthcare organizations operating across multiple facilities or supporting remote radiology teams, leveraging secure networks with distributed vpn locations can help maintain stable connections and strengthen protection for sensitive imaging data during transmission.
PACS interoperability at scale requires network infrastructure that can handle large DICOM datasets without packet loss, timeout failures, or retrieval queues that back up during peak hours.
PACS interoperability depends on all four components exchanging data through open standards. When any component defaults to proprietary interfaces, the integration chain requires custom middleware to compensate — and that middleware becomes a maintenance liability at every upgrade.
What are the four levels of interoperability, and where does PACS fit?
Healthcare interoperability is defined in four levels by HIMSS (Healthcare Information and Management Systems Society). Each level describes a deeper degree of integration. PACS interoperability spans all four levels, and understanding where a specific PACS implementation sits helps identify which gaps need to be closed.
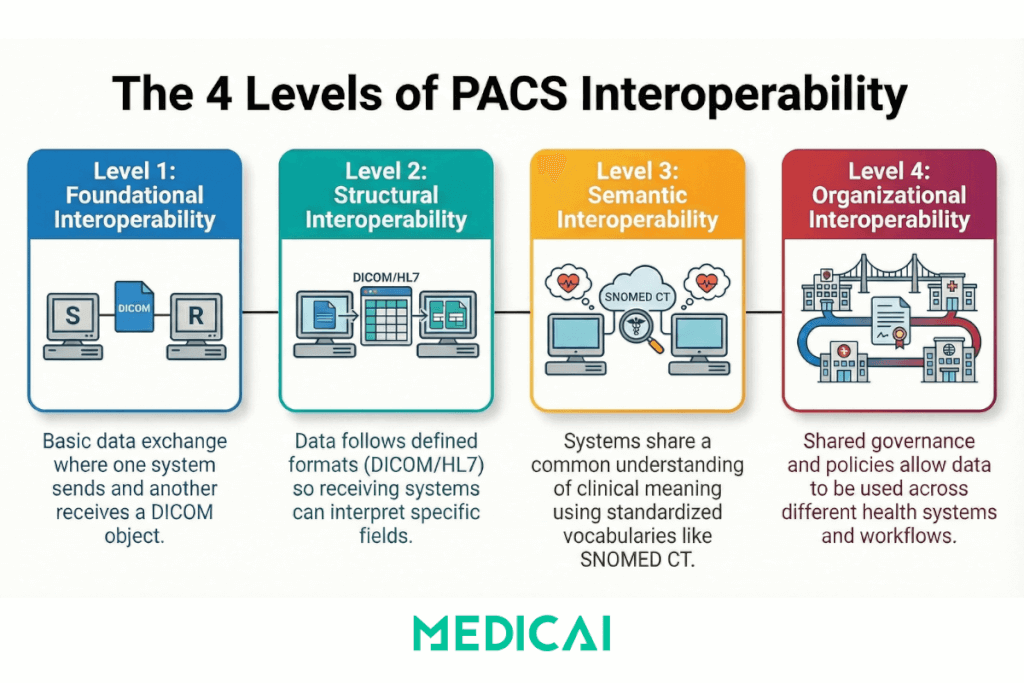
Level 1 — Foundational interoperability
Foundational interoperability means two systems can exchange data — one can send, the other can receive — without either system being required to interpret or use the data in any defined way. In PACS terms, foundational interoperability is achieved when a modality can successfully transmit a DICOM object to an archive. The data moves. Whether it lands under the correct patient, in the correct study, linked to the correct order — those belong to higher levels.
Level 2 — Structural interoperability
Structural interoperability means the format and syntax of the data are defined and consistent so that receiving systems can interpret the data at the field level. DICOM is the structural interoperability standard for imaging: it defines how imaging objects are constructed, how metadata fields are labeled, how series are grouped within studies, and how SOP Instance UIDs keep objects uniquely addressable. HL7 v2 provides structural interoperability for clinical messaging — defining message segments like PID for patient identity and OBR for order context. Structural interoperability is where most PACS integration failures originate: mismatched accession numbers, inconsistent patient identifiers, and non-standard private tags that importing systems cannot parse.
Level 3 — Semantic interoperability
Semantic interoperability means that systems not only exchange and interpret data structurally but also share a common understanding of what the data means. In PACS, semantic interoperability becomes relevant when imaging data crosses system boundaries and must be understood in a clinical context. A structured radiology report uses SNOMED CT, LOINC, and RadLex to ensure that a finding described in one system means the same thing in the receiving system. FHIR resources support semantic interoperability by providing standardized vocabulary bindings alongside data exchange, so that a FHIR ImagingStudy resource carries not just the study location but meaningful context about modality type, body part, and reason for study that downstream systems can act on without manual translation.
Level 4 — Organizational interoperability
Organizational interoperability is the highest level and extends beyond technical standards into governance, policy, and workflow. It means that different organizations — hospitals, health systems, teleradiology providers, payers, and outpatient imaging centers — can exchange data and actually use it within their own workflows, subject to shared governance agreements, consistent data stewardship policies, and compatible access controls. Organizational interoperability in PACS determines whether a referring physician at an affiliated hospital can open a prior study from a different site within their own EHR, or whether they still need to call the radiology department to request a CD. The technical plumbing can be perfect at levels one through three; organizational interoperability fails when governance, consent policies, or cross-entity trust agreements are not in place.
Most PACS implementations achieve foundational and structural interoperability. Semantic and organizational interoperability remain the harder problems — and the ones that have the greatest direct impact on clinical outcomes and care continuity.
Which standards power PACS interoperability?
PACS interoperability depends on a standards stack that separates imaging objects, clinical messaging, and modern API access.
PACS interoperability standards fall into three core groups.
- DICOM and DICOMweb, imaging objects and imaging transport
- HL7 v2, clinical messaging for demographics, orders, and results in many hospitals
- FHIR, web-first APIs for patient-context integration and app ecosystems
What does DICOM standardize for PACS interoperability?
The DICOM standard standardizes how imaging objects are stored, identified, moved, and retrieved across imaging systems.
DICOM supports the basic operations clinicians use daily.
- Store, images, and related objects land in the archive consistently
- Query and retrieve, study search, and priors access behave predictably
- Object identity, SOP Instance UIDs, and metadata keep studies addressable across systems
What does DICOMweb add to PACS interoperability?
DICOMweb adds REST-based access to the same DICOM objects found in .dcm files, and that shift suits browsers, cloud services, and modern integrations.
DICOMweb core services map to three clinical actions.
- QIDO-RS, query studies, and series for worklists and timelines
- WADO-RS, retrieve instances for viewing and downstream processing
- STOW-RS, store instances into an archive through web workflows
What does HL7 v2 carry in PACS interoperability?
HL7 v2 carries the clinical and administrative context that keeps images connected to the right patient and the right encounter.
HL7 v2 message categories map to common imaging problems.
- ADT, demographic, and encounter updates that prevent patient mismatches
- ORM, orders, and scheduling context that prevent orphan studies
- ORU, results delivery that prevents reportsfrom getting stuck outside the chart
What does FHIR change in PACS interoperability?
FHIR improves PACS interoperability by making patient-context integration and data access look like modern web APIs rather than interface-only plumbing.
FHIR helps when the goal is chart-native access. FHIR patterns support EHR launch context, consistent identity retrieval, and tighter app integration governance through authentication and authorization controls.
IHE Integration Profiles
DICOM defines how imaging objects are structured and transported. HL7 defines how clinical messages carry patient identity, orders, and results. What neither standard specifies on its own is the exact sequence of transactions that must occur, between which systems, in which order, to successfully complete a defined clinical workflow.
IHE — Integrating the Healthcare Enterprise — fills that gap. IHE is not a standards body in the sense that it does not write DICOM or HL7. It is a healthcare IT coordination initiative that produces integration profiles: use-case-specific rulebooks that specify which DICOM and HL7 transactions must occur, which systems must participate as defined actors, and what each actor is required to send or accept at each step.
The distinction matters for troubleshooting. Most interoperability failures in radiology IT are not DICOM nonconformance failures—the system sends valid DICOM. They are IHE profile non-conformance failures: the system sends DICOM in the wrong transaction sequence, skips a required actor grouping, or omits a field mandated by the profile even though the DICOM standard marks it optional. A PACS that passes DICOM conformance testing can still fail in a workflow because it was never tested against the IHE profile that governs that workflow.
What an IHE integration profile is
Every IHE integration profile defines three structural components.
- Actors — the system roles that participate in the workflow. Examples: Image Manager, Order Filler, Acquisition Modality, Report Creator, Document Registry.
- Transactions — the specific messages that flow between actors. Each transaction invokes a defined standard — a specific DICOM service or a specific HL7 message type — and specifies what fields are required, optional, or prohibited for that context.
- Actor groupings — requirements that a system claiming a particular actor role must also implement other profiles. A system acting as Document Registry in XDS-I.b must also implement Audit Trail and Node Authentication (ATNA). The grouping requirement is where security and identity obligations attach to workflow profiles.
The practical difference between DICOM conformance and IHE profile conformance is specificity. A DICOM conformance statement says a system can perform C-FIND. An IHE profile states that, when acting as the Acquisition Modality actor in Scheduled Workflow, the system must issue a specific C-FIND query to the Worklist Manager actor, using a defined set of matching keys in a defined sequence, triggered by a defined HL7 order message. One describes capability. The other describes behavior in a specific clinical workflow context.
The five IHE radiology profiles that govern this cluster
IHE publishes over 40 integration profiles in its Radiology Technical Framework. The table below covers only the profiles that appear by name in the Modality Worklist, PACS Migration, VNA, and PACS Interoperability guides. This is a working reference for the terminology in those posts, not a comprehensive IHE profile catalog.
| Profile | Abbreviation | What it governs | Where it appears in cluster |
|---|---|---|---|
| Scheduled Workflow | SWF / SWF.b | The complete ordering-to-image loop: order creation in HIS/RIS → Modality Worklist query at the scanner → image acquisition → DICOM store → study routing → viewing. | Modality Worklist guide; PACS workflow section |
| Patient Information Reconciliation | PIR | How PACS handles unidentified patients — trauma and emergency admissions — and reconciles images to the correct patient identity once established. | PACS Migration guide (identity reconciliation) |
| Cross-Enterprise Document Sharing for Imaging | XDS-I.b | How imaging studies are shared across enterprise or institutional boundaries using a document registry and repository model. | VNA guide (cross-enterprise retrieval); PACS Migration guide |
| Radiation Exposure Monitoring | REM | How dose data from CT and fluoroscopy is captured in DICOM Radiation Dose Structured Reports and shared consistently across systems. | PACS Migration guide (private tag and dose data handling) |
| Audit Trail and Node Authentication | ATNA | Security baseline: every system participating in an IHE profile environment must comply with ATNA. XDS-I.b explicitly requires it as a grouped profile. | VNA guide (security grouping requirement) |
IHE conformance versus DICOM conformance — what the difference means for interoperability failures
The HIMSS Level 2 definition — structural interoperability — describes systems that exchange data in a consistent, parseable format. Most radiology systems achieve Level 2. The failure mode that IHE profiles address is not format failure; it is workflow-sequence failure that produces structurally valid but clinically incorrect data.
Consider private tag data loss in a PACS migration. The migrated DICOM objects are structurally valid. The receiving archive parses them without error. The failure is that the receiving system’s DICOM Store actor was not configured to the profile behavior that preserves or maps private tag content during ingest, because no IHE profile mandated that behavior in the migration workflow, and nobody tested for it. The data moved at Level 2. It failed at Level 3 because meaning was lost.
The same pattern applies to identity reconciliation failures. Images of an unidentified trauma patient are uploaded to the archive under a temporary identifier. The images and the identifier are structurally valid DICOM. The failure occurs when the Patient Information Reconciliation profile’s transaction sequence — the one that triggers identity update propagation from the ADT system back to already-stored studies — was never implemented by the receiving PACS vendor, or was implemented but not activated in that environment’s configuration.
When a PACS vendor’s conformance documentation lists IHE profile support, the relevant questions are not only which profiles are listed, but which actors within each profile the vendor supports, and whether Connectathon testing results exist for those actor-transaction combinations. A vendor can list SWF support while implementing only the Acquisition Modality actor, leaving the Image Manager and Report Manager actors — the components that close the ordering loop back to the RIS — untested in a multi-vendor environment.
IHE Connectathon as a conformance signal
IHE holds an annual Connectathon — a structured testing event where vendors demonstrate that their systems correctly implement specific IHE profiles in live, multi-vendor integration tests. A Connectathon result is materially different from a self-attested conformance statement: it is documented, third-party-witnessed evidence that a specific version of a vendor’s system exchanged the correct transactions with other vendors’ systems acting in the defined actor roles.
For procurement and due diligence, Connectathon results are available publicly through the IHE Gazelle tool. When evaluating a PACS or VNA for an environment where SWF, XDS-I.b, or PIR are operationally relevant, checking Gazelle for that vendor’s most recent results for those specific profiles — and the specific actor roles within each profile — provides a verifiable baseline that conformance statements alone cannot.
The absence of a Connectathon result for a profile a vendor claims to support is not proof of non-conformance, but it shifts the testing burden to the integration project itself. In environments where IHE profile compliance is operationally critical, requiring documented Connectathon results for relevant profiles is a reasonable procurement criterion.
How does PACS enable interoperability in real clinician workflows?
PACS interoperability enables a consistent workflow loop, from acquisition to interpretation to distribution, without identity drift.
PACS interoperability shows up in six workflow handoffs.
- Registration and scheduling handoff, patient identity, and exam context get created upstream
- Modality worklist handoff, scheduled exams, and reduce manual demographic entry at acquisition
- Acquisition to archive handoff, images land in the right patient container
- Priors access handoff, prior studies become searchable and retrievable at reading time
- Reporting handoff, report objects, and results statuses return to the enterprise systems
- Distribution handoff, referrers, and care teams access images inside the chart
PACS interoperability success looks like stable patient matching, stable study links in the EHR, and predictable availability of priors across sites.

How do PACS help interoperability beyond standards?
PACS helps interoperability by acting as the operational broker between imaging production systems and clinical consumption systems.
PACS interoperability support from PACS falls into four roles.
- Normalization role, PACS enforces consistent metadata fields and identifiers at ingest
- Routing role, PACS controls where studies go, who sees them, and when priors arrive
- Context role, PACS aligns images to orders, encounters, and report states
- Distribution role, PACS delivers controlled access to viewers, EHR launch points, and external collaborators
PACS interoperability breaks when PACS is used only for storage. PACS interoperability works when PACS acts as a workflow infrastructure, not a passive vault.
What key benefits does PACS interoperability deliver?
PACS interoperability benefits cluster into measurable workflow and patient-safety outcomes.
PACS interoperability benefits include five outcomes.
- Comprehensive patient view, clinicians see images next to history, labs, and notes inside the EHR
- Workflow efficiency, fewer manual entries, and fewer “missing context” interruptions
- Faster reporting cycles, smoother handoffs from acquisition to signed report delivery
- Remote access and teleradiology, secure collaboration across sites without file shipping
- Continuity of care, priors stay reachable across years, sites, and vendor changes
PACS interoperability reduces repeat work.
PACS interoperability reduces repeats by keeping priors discoverable and by reducing identity errors that trigger re-acquisition.
What major challenges block PACS interoperability?
PACS interoperability challenges fall into three categories: vendor, technical, and governance constraints.
How does vendor lock-in limit PACS interoperability?
Vendor lock-in limits PACS interoperability when proprietary formats, private tags, or restricted export paths trap data and workflow behaviors within a single vendor stack.
Vendor lock-in creates predictable operational pain.
Vendor lock-in shows up during migrations, mergers, cross-site reads, and enterprise archive consolidation.
How do identity and metadata issues break PACS interoperability?
Identity and metadata issues break PACS interoperability when patient identifiers, accession numbers, or encounter context diverge between systems.
Identity failures produce clinical and operational symptoms.
- Wrong priors attached to the chart
- Orphan studies that never match an order
- Duplicate patient records that split the imaging history
- Broken EHR links that send clinicians back to phone calls
How do network and performance constraints block PACS interoperability?
Network and performance constraints hinder PACS interoperability when bandwidth and latency slow retrieval, streaming is unstable, or peak-hour performance is unpredictable.
Performance problems manifest as workflow issues.
Performance problems show up as slow priors access, stalled viewers, and reading backlogs.
How do security and compliance requirements shape PACS interoperability?
Security and compliance shape PACS interoperability because every new integration expands the access surface for ePHI.
Security controls that matter in PACS interoperability stay practical.
Access control, audit logging, encryption in transit and at rest, and least-privilege roles reduce risk without breaking workflow.
Why does governance decide PACS interoperability outcomes?
Governance decides PACS interoperability outcomes because standards support still varies by vendor, version, and configuration.
Governance work includes three ongoing tasks.
- Conformance review, what the vendor actually supports
- Interface monitoring, what fails in production, and how fast it gets fixed
- Change control, what breaks when systems are upgraded or add new sites
What emerging trends are shaping PACS interoperability?
PACS interoperability trends shift the center of gravity toward web access, enterprise-wide imaging, and tighter workflow automation.
Emerging trends in PACS interoperability include six shifts.
- DICOMweb-first access, browser viewers, and web integrations become the default
- Cloud and hybrid deployment patterns, object storage, and elastic scaling reshape retrieval expectations
- VNA and enterprise imaging patterns, archives decouple from viewers to reduce migration debt
- API-first integration expectations, FHIR-based context, and app launches get written into requirements
- AI in the workflow, AI outputs need to land inside the reading workflow with a traceable context
- Security hardening as baseline, resilience planning assumes ransomware events and credential abuse
PACS interoperability trend pressure lands in procurement.
PACS interoperability trend pressure lands in conformance statements, API availability, audit evidence, and measurable retrieval performance under load.
What to validate before you call PACS interoperability “done”?
PACS interoperability is achieved when clinical users no longer notice the integrations.
PACS interoperability validation checks cover five questions.
- Patient matching, does every study land under the right patient after upstream edits
- Order linkage, does every study reconcile to an order or scheduled context
- Priors access, do priors appear fast enough during peak reading hours
- Report delivery, does the report status land in the chart reliably
- Auditability, do logs prove who accessed what and when across systems
What is PACS now called, and does the term still apply?
In 2021, the U.S. Food and Drug Administration reclassified Picture Archiving and Communication Systems under a new device classification called Medical Image Communication and Management Systems, or MIMPS. The regulatory intent was to create a classification that better reflected the expanded scope of modern imaging infrastructure — which now includes cloud delivery, AI integration, enterprise-wide archive management, and cross-site distribution — capabilities that a definition built around the concept of a “picture archive” no longer fully described.
In practice, PACS remains the dominant term across clinical operations, procurement, radiology informatics, and vendor marketing. Radiologists, IT teams, and health system executives continue to use PACS as the working vocabulary for the imaging infrastructure layer. The MIMPS classification matters most in regulatory filings, FDA 510(k) clearance documentation, and compliance contexts where the formal device classification applies.
For interoperability purposes, the term change does not alter the underlying standards, integration patterns, or workflow requirements. Whether a vendor calls their product a PACS, an enterprise imaging platform, a VNA, or an imaging management system, the same interoperability standards apply: DICOM for imaging objects, HL7 v2 for clinical messaging, FHIR for API-based integration, and DICOMweb for web-native access. The obligation to achieve reliable patient matching, consistent study routing, and predictable priors retrieval does not change with the regulatory label.
If you encounter the MIMPS designation in a vendor’s regulatory documentation or a compliance audit, it refers to the same class of system this content addresses throughout. The interoperability requirements remain identical.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo