MRI Segmentation With AI: Multi-Organ Applications and Methods

MRI segmentation with AI converts raw magnetic resonance imaging data into labeled maps of anatomy and pathology that clinicians and researchers can measure, monitor, and analyze quantitatively. The underlying technology is consistent across all clinical contexts: deep learning models, primarily based on the U-Net architecture, learn to identify tissue boundaries and pathological regions from training data and then generate segmentation outputs in seconds, rather than the hours required by manual contouring.
The clinical applications vary significantly across organ systems. Brain MRI segmentation supports neurological diagnosis and surgical planning. Cardiac MRI segmentation enables calculation of ejection fraction and characterization of myocardial tissue. Liver MRI segmentation underpins hepatocellular carcinoma detection and fat quantification. Tumor segmentation across organs supports treatment response monitoring and oncologic surgical planning. Musculoskeletal segmentation enables cartilage quantification and orthopedic surgical guidance.
This guide covers the technical foundations, methodological evolution, and clinical applications of MRI segmentation across these five major clinical contexts.
What is MRI segmentation with AI?
MRI segmentation with AI is the process of using deep learning models to automatically divide an MRI scan into distinct, labeled regions representing specific tissue types, anatomical structures, or pathological areas. The output is a labeled map in which every voxel in the original scan is assigned to a specific category: gray matter or white matter for brain imaging; left ventricle or right ventricle for cardiac imaging; tumor core or peritumoral edema for oncologic imaging; and so on. The labeled output enables quantitative measurement, longitudinal tracking, and population-scale research that grayscale image interpretation alone cannot support efficiently.
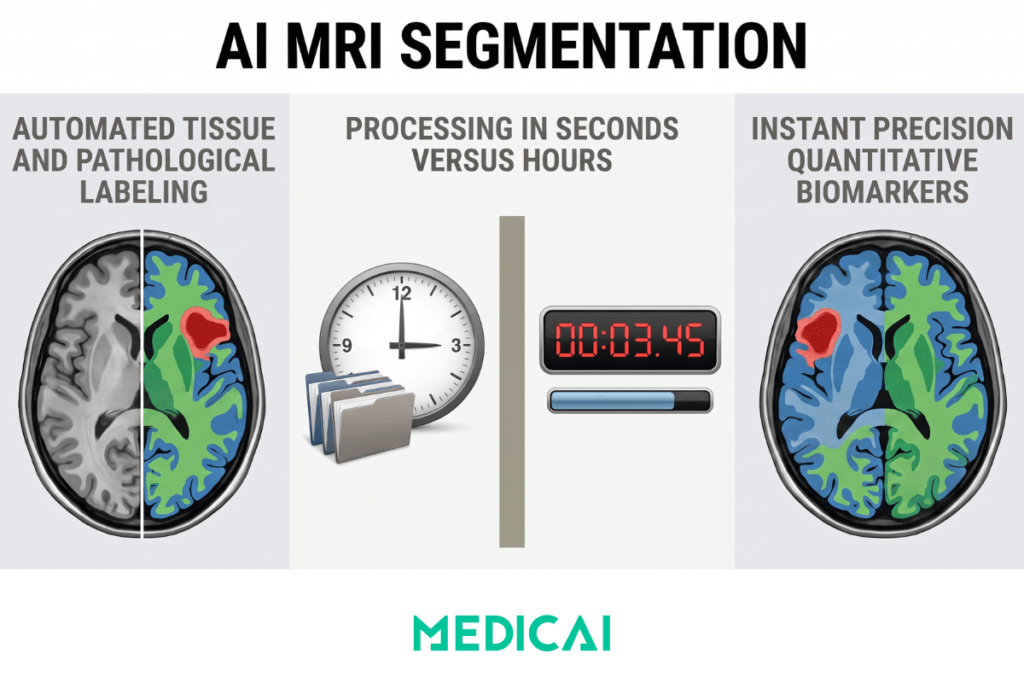
AI segmentation differs from manual segmentation by automating what was historically expert-performed work. A trained neuroanatomist or cardiac radiologist might spend 30 minutes to several hours per scan generating manual segmentations of complex anatomy. An AI segmentation model produces output in seconds to minutes, with accuracy that meets or exceeds the variability of experts on standard benchmark tasks across many clinical contexts. The shift from manual to AI segmentation represents one of the most consequential changes in medical imaging over the past decade.
The clinical value extends beyond raw speed. AI segmentation enables population-scale research that would be infeasible with manual contouring across hundreds of thousands of scans. It supports real-time quantitative measurements during radiology reads that previously required separate post-processing workflows. It allows longitudinal comparisons across imaging studies where consistent manual segmentation would be impractical. It surfaces quantitative biomarkers, tumor volume changes, cardiac ejection fraction, liver fat fraction, cartilage thickness, that increasingly drive clinical decision-making in cancer care, cardiology, hepatology, and orthopedics.
The remainder of this guide covers how MRI segmentation works in technical terms, how traditional methods evolved into modern AI approaches, and how segmentation is applied across the five major clinical contexts in which MRI plays a central role. The audience is healthcare technical leadership and clinical AI evaluators researching segmentation capabilities for clinical deployment or technology evaluation.
Why AI is transforming MRI segmentation
The shift from traditional segmentation methods to AI-based approaches is driven by three structural factors that compound in clinical impact.
The first factor is accuracy improvement on objective benchmarks. Modern deep learning models trained on properly preprocessed MRI data achieve Dice similarity scores of 0.85-0.95+ on standard benchmark datasets for brain, cardiac, liver, and tumor segmentation tasks. Traditional methods typically achieved 0.70-0.85 on the same benchmarks. This accuracy improvement is not marginal; it crosses the threshold at which segmentation outputs become clinically usable for quantitative measurement without manual correction.
The second factor is speed and scalability. A trained AI segmentation model processes a typical MRI study in seconds to minutes on modern GPU infrastructure. Manual segmentation of the same study takes 30 minutes to several hours, depending on complexity. This speed difference enables clinical workflows that were previously impractical, real-time quantitative measurement during radiology reads, longitudinal volume tracking across years of patient imaging, and population-scale research drawing on biobank initiatives with hundreds of thousands of scans.
The third factor is consistency and reproducibility. Manual segmentation introduces inter-rater variability that can exceed 10-15 percent for complex segmentation tasks. AI segmentation produces identical outputs given identical inputs, eliminating one source of variability in quantitative imaging biomarkers. This consistency matters enormously for clinical research, where small effect sizes can be obscured by measurement noise, and for clinical care, where treatment decisions depend on small changes in measured parameters.
These three factors compound. Accuracy, speed plus consistency together produce clinical workflows and research applications that did not exist a decade ago. Cancer treatment response monitoring with regular volumetric measurements. Cardiac ejection fraction calculation is integrated directly into reading workflows. Population-scale brain atrophy tracking for clinical trials. Real-time orthopedic surgical planning with quantitative cartilage assessment. The AI segmentation transition is not just about better technology; it is about new clinical capabilities becoming operationally viable.
Technical foundations of MRI segmentation
MRI segmentation begins with understanding image dimensions and data quality limitations. The same technical foundations apply across brain, cardiac, liver, tumor, and musculoskeletal segmentation tasks, with organ-specific protocol differences in the details rather than the underlying framework.
Image dimensions affect both segmentation accuracy and computational cost. MRI data comes in two structural forms. Two-dimensional slices represent single-plane images, commonly used in clinical practice for their faster acquisition and simpler interpretation. Three-dimensional volumes represent full anatomical regions composed of stacked slices across multiple planes (axial, sagittal, coronal). 2D segmentation is faster and requires less computational power. 3D segmentation provides richer spatial context, which is particularly important for organs whose structures span multiple slices (brain, heart, liver), but it introduces challenges, including higher memory usage, longer training times, and the need for consistent preprocessing across slices.
Common MRI artifacts affect segmentation accuracy regardless of the organ. Noise represents random variation in voxel intensity, often due to a low signal-to-noise ratio in fast acquisition protocols. The partial volume effect occurs when a voxel contains more than one tissue type, blurring boundaries that segmentation models must learn to handle. The bias field (intensity inhomogeneity) is a gradual shading artifact that makes the same tissue appear brighter in one region and darker in another, particularly problematic for tissue-class segmentation. Motion artifacts affect the segmentation of all organs that move during acquisition, with cardiac and abdominal imaging more affected than brain imaging. These artifacts can degrade even well-designed segmentation models, which is why preprocessing is essential.
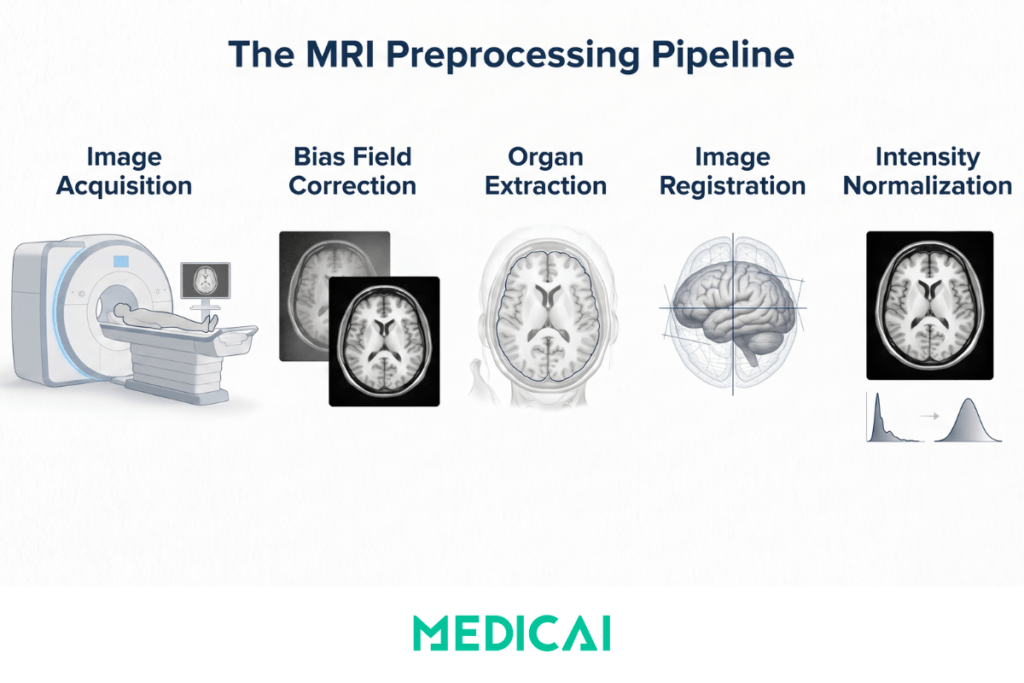
A standard preprocessing pipeline for MRI segmentation includes five steps applied in sequence.
Image acquisition collects the raw MRI data in the sequences appropriate to the clinical question — T1-weighted, T2-weighted, FLAIR, diffusion-weighted, contrast-enhanced, or quantitative mapping sequences, depending on the organ and clinical context.
Bias field correction addresses intensity inhomogeneity using algorithms like N4ITK (Nonparametric Nonuniform Intensity Normalization), which is the most widely used implementation across organs.
Organ extraction isolates the target anatomy from surrounding tissue. For brain MRI this is skull stripping using tools like BET (Brain Extraction Tool in FSL) or SPM tissue masks. For liver imaging, the goal is to isolate the liver parenchyma from surrounding abdominal organs. In cardiac imaging, this involves isolating the heart within the chest. Each organ has its own established tools and approaches.
Image registration aligns scans to a standard reference space when needed, typically using tools like FSL FLIRT or ANTs. Registration matters most for population-scale studies and longitudinal comparisons where consistent anatomical alignment is required.
Intensity normalization standardizes voxel intensities across subjects or sessions to reduce variability that would otherwise confuse segmentation models. Common approaches include histogram matching, z-score normalization, and percentile-based scaling.
Modern AI segmentation pipelines often integrate preprocessing steps into the model architecture, but the underlying principles of preprocessing remain. Models trained without proper preprocessing show reduced generalization to new clinical sites and protocols, which is one of the most common reasons for AI segmentation performance to degrade between research validation and clinical deployment.
Traditional vs AI segmentation methods
MRI segmentation evolved through three distinct methodological eras: manual segmentation by experts, classical computational methods, and modern deep learning approaches. Each era contributed methods that remain in use for specific applications.
Manual segmentation by trained experts is the historical gold standard and remains essential for creating training datasets and validating new methods. A neuroanatomist or radiologist outlines anatomical structures or pathological regions, slice by slice, using specialized software such as ITK-SNAP, 3D Slicer, or domain-specific tools. The accuracy of expert manual segmentation defines the upper bound that AI segmentation models attempt to match. The limitations are slow throughput (30 minutes to several hours per scan), inter-rater variability (different experts produce different segmentations of the same scan), and the inability to scale to large datasets.
Classical computational methods emerged through the 1990s and 2000s as approaches to automate parts of the manual workflow. Thresholding selects intensity values that separate tissue classes, working well when contrast is high but failing when intensities overlap. Region growing starts from a seed point and expands regions by adding similar-intensity neighbors; it is useful for connected structures but sensitive to seed placement. K-means clustering groups voxels in feature space based on intensity, providing fast unsupervised segmentation but assuming uniform cluster shapes. Fuzzy C-means clustering allows partial membership across multiple classes, better handling partial volume effects than hard clustering. Atlas-based segmentation registers pre-labeled probabilistic brain atlases to patient scans, transferring labels through the registration, which works well for normal anatomy but struggles with deformed anatomy.
Deep learning methods, dominated by the U-Net architecture, have largely superseded classical methods for clinical segmentation tasks since 2015. U-Net was introduced in 2015 by Ronneberger, Fischer, and Brox at the University of Freiburg for biomedical image segmentation. The architecture uses a symmetrical encoder-decoder structure: the encoder progressively reduces spatial resolution while extracting features; the decoder progressively reconstructs spatial resolution while predicting class labels at each voxel; and skip connections preserve fine-grained spatial detail from the encoder to the decoder. U-Net works well with relatively small training datasets (thousands rather than millions of examples), produces pixel-precise segmentation maps, and adapts to both 2D and 3D inputs.
Modern variants significantly extend the original U-Net architecture. nnU-Net (no-new-U-Net) is a self-configuring framework that automatically adapts U-Net to new datasets, providing strong baseline performance across diverse segmentation tasks. 3D U-Net variants handle volumetric data directly rather than processing 2D slices. Attention U-Net incorporates attention mechanisms that focus on relevant image regions. Transformer-based architectures (TransUNet, Swin-UNet) integrate transformer attention with the U-Net structure. The MONAI framework provides healthcare-specific implementations of these architectures with established preprocessing and training utilities.
| Dimension | Traditional Methods (Pre-2015) | Deep Learning Methods (Post-2015) |
|---|---|---|
| Core approach | Hand-engineered features, thresholding, region growing, atlas registration, classical clustering | Learned features via convolutional neural networks, primarily U-Net and its variants |
| Training data required | None for unsupervised methods, small annotated sets for atlas-based approaches | Annotated training data required, typically hundreds to thousands of expert-segmented scans |
| Processing time | Minutes to hours per scan, depending on method and parameters | Seconds to minutes per scan after model training is complete |
| Handling of variability | Sensitive to noise, bias field, partial volume effects, and anatomical variation | Robust to variability when trained on diverse data, generalizes across protocols and populations |
| Accuracy on benchmarks | Dice scores typically 0.70 to 0.85 on standard brain segmentation tasks | Dice scores typically 0.85 to 0.95+ on the same benchmarks with modern U-Net variants |
| Common tools | FreeSurfer, FSL FAST, SPM, ANTs, manual outlining with ITK-SNAP | QuickNAT, SynthSeg, nnU-Net, MONAI framework, commercial AI tools |
| Best for | Research with limited training data, well-characterized anatomy, ground-truth dataset generation | Clinical deployment, real-time workflows, multi-institutional and multi-protocol settings |
MRI segmentation across clinical contexts
The technical foundations and methodological approaches covered above apply consistently across every clinical MRI segmentation context. The specific applications, benchmark datasets, clinical reporting frameworks, and quantitative measurements differ by organ system. The five clinical contexts below account for most of the current research activity and commercial AI segmentation deployments.
Brain MRI segmentation
Brain MRI segmentation supports neurological diagnosis, surgical planning, and quantitative neuroscience research across three categories of segmentation tasks.
Tissue segmentation separates the brain into gray matter, white matter, and cerebrospinal fluid. Gray matter contains the densely packed neurons that process information. White matter contains the nerve fibers that connect brain regions. Cerebrospinal fluid surrounds and protects the brain and spinal cord. Quantitative measurements derived from tissue segmentation support studies of brain development, aging, and neurological disorders. Brain atrophy tracking in Alzheimer’s disease, white matter lesion quantification in multiple sclerosis, and gray matter volume measurement in psychiatric research all depend on accurate tissue segmentation.
Pathological segmentation identifies abnormal regions, including tumors, edema, lesions from stroke or multiple sclerosis, and other focal brain abnormalities. The clinical applications include diagnosis, surgical planning for tumor resection, radiation therapy target delineation, and treatment response monitoring through volumetric tracking. Glioma segmentation is the most extensively researched pathological brain segmentation task, with the BRATS Challenge driving methodological progress since 2012.
Anatomical segmentation divides the brain into specific regions, including lobes (frontal, temporal, parietal, occipital), cortical areas, ventricles, and deep gray nuclei (thalamus, putamen, hippocampus, amygdala). Surgical navigation, functional connectivity research, and structural biomarker development in psychiatric disorders all depend on accurate anatomical segmentation. Hippocampal volume is particularly important as a biomarker in Alzheimer’s disease research and clinical assessment.
The dominant tools for brain MRI segmentation reflect this taxonomy. FreeSurfer and FSL FAST remain widely used for tissue and anatomical segmentation in research, particularly in studies that require established processing pipelines with extensive prior validation. QuickNAT provides fast, deep learning-based brain segmentation as a research tool. SynthSeg is notable for working across different MRI contrasts and sequences without requiring sequence-specific training data, making it useful for retrospective studies pooling data from multiple sources. Commercial AI tools have emerged across brain tumor segmentation (used in radiation oncology planning) and structural segmentation for clinical research applications.
The benchmark datasets driving research progress include BrainWeb (simulated brain MRIs with known ground truth), IBSR (Internet Brain Segmentation Repository, providing expert-annotated real human MRI scans), BRATS for tumor segmentation, and population-scale datasets such as OASIS and ADNI, which provide annotated data for clinical research tool development. Validation against these benchmarks, using the Dice coefficient, Jaccard index, and Hausdorff distance, is the standard methodology. Modern deep learning approaches consistently achieve Dice scores in the 0.85-0.95 range across these benchmarks, with the best models approaching the ceiling of inter-rater variability in expert manual segmentation.
Clinical deployment of brain AI segmentation has progressed unevenly across applications. Tumor segmentation for radiation therapy planning is mature with multiple FDA-cleared products. Structural brain volume measurement for clinical use in dementia evaluation is emerging through several commercial tools. Real-time segmentation integrated into routine radiology reading remains uncommon, with adoption typically driven by neuroscience research programs at academic medical centers rather than in community radiology settings.
Cardiac MRI segmentation
Cardiac MRI segmentation extracts the four heart chambers, myocardial walls, and pathological tissue regions from cardiac magnetic resonance studies, enabling quantitative measurement of cardiac function and tissue characterization that would otherwise require time-intensive manual contouring by cardiology specialists.
The clinical applications cluster around three workflows that depend on different MRI sequences. Cardiac function assessment uses cine MRI sequences captured throughout the cardiac cycle to measure ventricular volumes, ejection fraction, stroke volume, cardiac output, and wall motion abnormalities. Tissue characterization uses late gadolinium enhancement (LGE) imaging to identify myocardial scar from infarction, fibrosis, and inflammation. Quantitative tissue mapping uses native T1, T2, and extracellular volume (ECV) mapping sequences to quantify diffuse myocardial changes that focal segmentation alone cannot capture.
Each workflow places different demands on segmentation models. Cine MRI segmentation requires consistent labeling of the ventricles across multiple cardiac cycle phases, with temporal consistency between phases to enable accurate ejection fraction calculation. LGE segmentation requires distinguishing scar tissue from the surrounding normal myocardium, where the contrast difference can be subtle, and scar morphology varies dramatically across patients. Tissue-mapping segmentation requires accurate delineation of the myocardial wall for quantitative pixel-wise analysis. Modern cardiac AI platforms typically include either separate models for each workflow or unified architectures that handle all three, with workflow-specific output heads.
The dominant commercial platform for cardiac MRI quantitative analysis is Cvi42 by Circle Cardiovascular Imaging, which has become the de facto standard in academic and large hospital settings. Medis Suite by Medis Medical Imaging is widely deployed across both research and clinical cardiac MRI workflows. syngo.via Cardiac by Siemens Healthineers integrates with Siemens cardiac MRI scanners and provides AI-augmented segmentation directly in the reading workflow. AI-augmented modules from the major cardiac MRI vendors (GE, Philips, Siemens) integrate segmentation outputs into reading rather than requiring separate post-processing.
The benchmark datasets and challenges that drive research progress include the ACDC (Automated Cardiac Diagnosis Challenge) from MICCAI 2017, which provided standardized cardiac MRI data across normal subjects and pathological cases; the M&Ms (Multi-Center, Multi-Vendor and Multi-Disease) Challenge, which extended ACDC by adding data from multiple imaging centers and vendor systems to test generalization across the heterogeneous clinical environment; and the UK Biobank cardiac MRI dataset, which provides population-scale training data from tens of thousands of participants with longitudinal follow-up. Recent research literature on cardiac segmentation is dominated by nnU-Net implementations and customized 3D U-Net variants that handle the spatial-temporal nature of cine sequences.
Clinical integration of cardiac AI segmentation has progressed significantly over the past five years. Several FDA-cleared and CE-marked cardiac MRI AI products now include segmentation modules that produce ejection fraction, ventricular volumes, and ECV measurements directly in the radiologist’s reading environment. Adoption has been fastest in academic medical centers and large cardiac MRI programs where quantitative measurements support clinical research alongside routine care. Smaller cardiac MRI programs typically adopt segmentation tools through their existing PACS or cardiology image analysis platforms.
The remaining challenges in cardiac MRI segmentation include handling extreme pathological cases (severe dilated cardiomyopathy, complex congenital heart disease) where training data is limited, generalizing across the multi-vendor environment where MRI sequences vary in subtle ways, and validating segmentation accuracy against the gold standard of expert manual contouring in cases where the manual ground truth itself has measurable inter-rater variability. Active research continues across all three challenge areas, with progress particularly visible in the M&Ms Challenge follow-up iterations.
Liver MRI segmentation
Liver MRI segmentation supports lesion detection and characterization, anatomical mapping of the Couinaud segments for surgical planning, and quantitative tissue analysis for evaluating diffuse liver disease. Clinical demand has grown alongside the rise of hepatocellular carcinoma (HCC) surveillance protocols, non-alcoholic fatty liver disease (NAFLD) evaluation, and the increasing role of MRI as a non-invasive alternative to biopsy in hepatology.
Lesion segmentation covers hepatocellular carcinoma (the most common primary liver malignancy), metastases from extra-hepatic primary cancers (colorectal, breast, neuroendocrine, melanoma, and others), and benign lesions, including hemangiomas, focal nodular hyperplasia (FNH), and adenomas. Each lesion type has distinctive imaging characteristics across the standard MRI sequences used in liver imaging, and accurate segmentation enables both lesion identification and characterization for treatment planning.
Modern liver MRI protocols use multi-phase contrast-enhanced sequences that capture the differential vascular dynamics distinguishing lesion types. The arterial phase (acquired 20 to 40 seconds after contrast injection) shows tumors with arterial hypervascularity. The portal venous phase (60 to 90 seconds post-injection) shows normal hepatic parenchymal enhancement. The delayed phase (3 to 5 minutes post-injection) shows washout patterns that distinguish HCC from other lesion types. Hepatobiliary contrast agents, such as gadoxetate disodium, add a hepatobiliary phase (at 15 to 20 minutes) that further improves lesion characterization. AI segmentation models trained on multi-phase data outperform single-phase approaches because the temporal contrast information is itself diagnostic for many lesion types.
The clinical reporting framework that segmentation outputs feed into is the Liver Imaging Reporting and Data System (LI-RADS), which provides standardized criteria for HCC diagnosis based on imaging features, including arterial phase hyperenhancement, washout, capsule appearance, and threshold growth. AI segmentation supports LI-RADS reporting by automating volumetric measurements, tracking growth across longitudinal studies, and providing consistent lesion characterization, thereby reducing inter-reader variability.
Beyond focal lesion segmentation, quantitative liver MRI applications include proton density fat fraction (PDFF) measurement for steatosis quantification (the standard non-invasive measurement for NAFLD severity), R2-star or T2-star mapping for iron quantification in hemochromatosis and transfusion-dependent anemia, and MR elastography for liver stiffness measurement as a marker of fibrosis. AI segmentation of the liver parenchyma is the foundation for all three quantitative applications, with the segmentation defining the region of interest for pixel-wise quantitative analysis.
Anatomical segmentation of the eight Couinaud segments (the functional liver segments defined by portal vein and hepatic vein anatomy) supports pre-surgical planning for hepatic resection. AI segmentation of these segments allows surgeons to plan resection lines that preserve adequate functional liver volume while removing all tumor-containing tissue. This application is particularly important in living donor liver transplantation, where accurate volumetric calculation determines the safety of both donor and recipient.
The benchmark datasets driving research progress include the LiTS (Liver Tumor Segmentation) Challenge from MICCAI 2017, which remains the dominant benchmark for liver and liver tumor segmentation; and the CHAOS (Combined Healthy Abdominal Organ Segmentation) Challenge, which provides multi-organ training data, including liver, alongside spleen, kidneys, and other abdominal structures. Recent research literature is dominated by 3D U-Net architectures with attention mechanisms, with nnU-Net providing a strong baseline performance.
Clinical deployment of liver AI segmentation has been growing in academic medical centers and large hepatology programs. Several FDA-cleared products now integrate liver segmentation with LI-RADS reporting workflows. Applications for liver fat quantification and iron measurement are particularly mature, with multiple commercial products available for clinical use. The remaining adoption barriers include integration with hepatology-specific clinical workflows and validation of AI segmentation accuracy across the diverse imaging protocols used at different institutions.
Tumor segmentation across organs
Tumor segmentation extends beyond brain imaging to every organ system in which MRI plays a diagnostic role in oncology. The clinical pattern is consistent across organs: identify the tumor boundary, separate sub-regions (enhancing core, necrotic core, peritumoral edema, where applicable), measure volume, and track changes over longitudinal imaging studies to support assessment of treatment response.
The differences across organs lie in the specific anatomy, the MRI sequences used for characterization, and the clinical reporting frameworks that depend on segmentation outputs. The common framework for organ-specific tumor segmentation uses a multimodal MRI input comprising T1-weighted, T2-weighted, FLAIR, diffusion-weighted imaging (DWI), and contrast-enhanced sequences, processed with deep learning fusion architectures.
Brain tumor segmentation is the most extensively researched application, anchored by the BRATS (Brain Tumor Segmentation) Challenge that has run annually since 2012. The standard BRATS labels separate the whole tumor (everything visible on imaging), the tumor core (enhancing plus necrotic regions), and the enhancing tumor specifically. Treatment response is assessed using the RANO (Response Assessment in Neuro-Oncology) criteria, which rely on accurate volumetric measurements provided by segmentation. Recent BRATS iterations have added datasets covering pediatric brain tumors and meningiomas, expanding the methodological reach beyond adult glioma.
Prostate tumor segmentation uses the PROSTATEx Challenge data and supports PI-RADS (Prostate Imaging Reporting and Data System) clinical reporting. The multi-parametric MRI approach to prostate cancer evaluation combines T2-weighted imaging, diffusion-weighted imaging with apparent diffusion coefficient (ADC) maps, and dynamic contrast-enhanced sequences. AI segmentation supports lesion identification, biopsy targeting through fusion with transrectal ultrasound, and active surveillance monitoring for low-risk disease.
Breast tumor segmentation increasingly uses dynamic contrast-enhanced MRI sequences for tumor characterization, particularly in high-risk screening populations and treatment response monitoring for neoadjuvant chemotherapy. Datasets driving research include the TCIA Duke Breast Cancer MRI collection and the MAMA-MIA breast cancer MRI initiative. The clinical applications span screening, MRI interpretation, surgical planning for breast conservation versus mastectomy decisions, and neoadjuvant therapy response assessment using tumor volume changes.
Liver tumor segmentation builds on the LiTS Challenge described in the liver section above. The clinical applications focus on HCC characterization within LI-RADS, treatment response monitoring after locoregional therapy (transarterial chemoembolization, radioembolization, ablation), and pre-surgical planning for resection.
Treatment response assessment across organ-specific tumor segmentation uses different criteria depending on the clinical context. RECIST (Response Evaluation Criteria in Solid Tumors) is the general framework for solid tumor response, measuring change in the longest diameter of target lesions. mRECIST (modified RECIST) adjusts the framework for HCC by measuring viable enhancing tumor rather than the entire lesion, including necrotic regions. RANO covers neuro-oncology with its own modifications. PI-RADS for prostate and LI-RADS for liver provide organ-specific characterization frameworks. AI segmentation feeds all of these frameworks by providing the volumetric measurements that the criteria depend on.
Musculoskeletal MRI segmentation
Musculoskeletal MRI segmentation supports orthopedic surgical planning, sports medicine assessment, and quantitative tracking of degenerative conditions like osteoarthritis. The clinical applications cluster around five segmentation targets: cartilage, bone, muscle, meniscus, and ligaments, with each target serving different clinical workflows.
Cartilage segmentation in the knee is the most extensively developed musculoskeletal application, driven by the Osteoarthritis Initiative (OAI) dataset, which provides longitudinal MRI scans from thousands of participants over multiple years of follow-up. Quantitative measurements of cartilage thickness, volume, and T2 relaxation time derived from segmentation outputs support clinical research on osteoarthritis progression, treatment response in disease-modifying drug trials, and individual patient monitoring in advanced cases. Similar approaches apply to hip and shoulder cartilage segmentation, though with smaller dataset availability and less methodological maturity.
Bone segmentation feeds into orthopedic surgical planning, custom implant design, and 3D-printed surgical guides. Total knee arthroplasty, total hip arthroplasty, and complex shoulder reconstruction increasingly use patient-specific surgical guides designed from segmented MRI data. The segmentation supports preoperative planning, intraoperative guide design, and postoperative outcome assessment.
Muscle segmentation supports sarcopenia evaluation in aging populations and muscle injury assessment in sports medicine. Thigh muscle volume measured from MRI is increasingly used as a body composition biomarker in research on aging, cancer cachexia, and chronic disease. Sports medicine applications include hamstring injury characterization, calf muscle assessment after Achilles repair, and shoulder muscle evaluation in rotator cuff disease.
Meniscus segmentation and ligament segmentation support specific orthopedic diagnostic workflows. Meniscus tear characterization combines morphological segmentation with signal analysis to grade the severity of the tear. ACL segmentation supports reconstructive surgery planning, particularly in revision cases where prior surgical hardware affects imaging interpretation.
The musculoskeletal segmentation space is less benchmark-driven than brain or cardiac segmentation. Clinical adoption has been faster in surgical planning workflows than in routine diagnostic imaging, with surgical planning companies driving methodological development through commercial products rather than research challenges. nnU-Net and 3D U-Net architectures dominate current research, with commercial deployment growing through orthopedic-focused AI vendors that integrate segmentation outputs into surgical planning software rather than radiology reading workflows.
The remaining challenges include handling the diversity of MSK MRI protocols across institutions (which vary more than brain or cardiac protocols), validating accuracy against expert measurements that themselves have substantial inter-rater variability for some musculoskeletal structures, and integrating segmentation outputs with the orthopedic surgical workflow rather than the radiology reading workflow.
| Clinical Context | Primary Segmentation Targets | Benchmark Datasets | Clinical Reporting Framework |
|---|---|---|---|
| Brain | Gray matter, white matter, CSF, tumor sub-regions, anatomical structures | BrainWeb, IBSR, BRATS, OASIS, ADNI | RANO criteria for tumor response, volumetric atrophy tracking |
| Cardiac | Left and right ventricles, atria, myocardium, scar tissue from LGE | ACDC, M&Ms Challenge, UK Biobank cardiac MRI | Ejection fraction, ventricular volumes, ECV mapping |
| Liver | Liver volume, Couinaud segments, lesions, fat fraction, iron content | LiTS Challenge, CHAOS Challenge | LI-RADS for HCC characterization, PDFF for steatosis |
| Tumor (cross-organ) | Enhancing core, necrotic core, peritumoral edema, longitudinal volume tracking | BRATS, PROSTATEx, TCIA Duke Breast Cancer MRI, MAMA-MIA | RECIST, mRECIST, RANO, PI-RADS, LI-RADS by organ |
| Musculoskeletal | Cartilage, bone, muscle, meniscus, ligaments | OAI (knee), smaller hip and shoulder datasets | Cartilage thickness/volume tracking, sarcopenia indices |
Validation and benchmarks for MRI segmentation
Validation of MRI segmentation models depends on comparison against expert-annotated reference data using standardized metrics. The methodology is consistent across organs, even when the specific datasets and clinical relevance differ.
The dominant validation metric is the Dice similarity coefficient (DSC), which measures the overlap between the predicted segmentation and the ground truth as a ratio ranging from 0 (no overlap) to 1 (perfect overlap). Modern deep learning segmentation models achieve Dice scores of 0.85 to 0.95 across standard benchmarks for brain tissue, cardiac chambers, liver parenchyma, and major tumor types. Scores above 0.90 generally indicate clinically acceptable segmentation accuracy, though the threshold varies by application (some quantitative measurements require higher accuracy than others).
Complementary metrics provide different views on segmentation quality. The Jaccard index (intersection over union) reports overlap differently than Dice and is sometimes preferred for specific applications. The Hausdorff distance measures the maximum surface distance between the predicted and ground-truth boundaries, identifying cases where overall overlap is high but boundary placement has localized errors. Sensitivity (recall) and specificity capture different aspects of segmentation correctness for binary classification tasks. Pixel-wise accuracy is the simplest metric, but it can be misleading when class imbalance is large (a brain tumor segmentation that calls everything background can achieve 99 percent pixel accuracy while being clinically useless).
The standard benchmark datasets across organs include BrainWeb and IBSR for brain tissue, BRATS for brain tumors, ACDC and M&Ms for cardiac, LiTS for liver and liver tumors, OAI for knee cartilage, and PROSTATEx for prostate cancer. Each benchmark provides expert-annotated ground truth that segmentation models compete against. The benchmark scores published in research papers establish the performance ceiling for new methods.
For clinical deployment beyond research validation, additional validation steps matter: testing on data from sites not represented in training, evaluation across the diverse imaging protocols used clinically, and assessment of failure modes that may be rare in benchmark data but clinically important in deployment.
Clinical integration considerations for AI segmentation deployment
Clinical deployment of MRI segmentation AI requires considerations beyond model accuracy. The factors that determine whether a segmentation tool delivers value in real clinical environments include integration with existing imaging infrastructure, regulatory clearance and compliance, workflow fit, and validation across deployment-specific data.
Integration with PACS and reading workflows is foundational. Segmentation outputs that require radiologists to switch between separate applications create workflow friction, limiting adoption. Integration patterns that work include embedded segmentation in the PACS viewer, automatic segmentation triggered by study arrival with results pre-populated in the reading workflow, and integration with vendor-neutral archives that allow segmentation outputs to flow alongside the original DICOM data.
Regulatory clearance differs by clinical application and jurisdiction. FDA clearance in the United States and CE marking in Europe follow different pathways depending on the intended use, with the most stringent requirements for AI tools that make autonomous clinical decisions. Most current AI segmentation tools function as decision support, with radiologist verification of final findings, which fits a less stringent regulatory pathway than autonomous diagnostic AI.
Workflow fit determines whether segmentation tools save time or add overhead. Tools that produce outputs requiring extensive manual correction offer little value compared to manual segmentation. Tools that work autonomously in most cases, with quality-control flags for the minority of difficult cases, deliver the speed and consistency benefits that justify deployment.
Cross-site validation is essential because models trained on one institution’s data often degrade when deployed at sites with different imaging protocols, scanner vendors, or patient populations. Validation on deployment-specific data before clinical use, with ongoing monitoring after deployment, is increasingly considered standard practice.
Frequently asked questions about MRI segmentation with AI
MRI segmentation with AI is the process of using deep learning models to automatically divide an MRI scan into distinct, labeled regions representing specific tissue types, anatomical structures, or pathological areas. The output is a labeled map where every voxel is assigned to a specific category. AI segmentation produces results in seconds to minutes with accuracy that meets or exceeds expert variability on standard benchmarks across brain, cardiac, liver, tumor, and musculoskeletal applications.
Traditional MRI segmentation methods (thresholding, region growing, clustering, atlas-based approaches) use hand-engineered rules and statistical models to identify regions. AI methods, primarily U-Net and its variants, learn segmentation patterns directly from training data. AI typically produces faster results (seconds vs minutes), higher Dice scores on benchmarks (0.85 to 0.95+ vs 0.70 to 0.85), and better handling of imaging variability, but requires substantial annotated training data.
U-Net is a convolutional neural network architecture introduced in 2015 by Ronneberger, Fischer, and Brox at the University of Freiburg for biomedical image segmentation. It uses a symmetrical encoder-decoder architecture with skip connections that preserve spatial detail. U-Net works well with small training datasets, produces pixel-precise segmentation maps, and adapts to both 2D and 3D inputs. It has become the dominant architecture for medical image segmentation across brain, cardiac, liver, and tumor applications.
AI segmentation has been developed and clinically deployed across multiple organ systems. Brain MRI segmentation covers tissue classification, anatomical structures, and tumors. Cardiac MRI segmentation covers heart chambers, myocardium, and scar tissue. Liver MRI segmentation covers liver volume, Couinaud segments, lesions, and quantitative tissue characterization. Tumor segmentation extends across brain, prostate, breast, and liver. Musculoskeletal segmentation covers cartilage, bone, muscle, meniscus, and ligaments.
Modern AI MRI segmentation models achieve Dice similarity scores of 0.85 to 0.95+ on standard benchmark datasets across brain, cardiac, liver, and tumor segmentation tasks. The accuracy is sufficient for many clinical applications including quantitative measurement, treatment response monitoring, and surgical planning. Real-world clinical accuracy depends on training data quality, preprocessing pipeline robustness, and validation across the specific imaging protocols and patient populations used at the deployment site.
Standard MRI segmentation preprocessing includes bias field correction (N4ITK for intensity inhomogeneity), organ extraction (skull stripping for brain, liver parenchyma isolation for abdominal), image registration to standard space when needed (FSL FLIRT, ANTs), and intensity normalization across subjects. Without proper preprocessing, segmentation accuracy degrades significantly, particularly for deep learning models trained on preprocessed data. Modern AI pipelines often integrate preprocessing steps within the model architecture.
Brain MRI segmentation uses FreeSurfer, FSL FAST, QuickNAT, and SynthSeg for various applications. Cardiac MRI segmentation uses cvi42 by Circle Cardiovascular Imaging, Medis Suite, and syngo.via Cardiac. Liver segmentation uses both research tools and FDA-cleared commercial products integrated with LI-RADS workflows. Across organs, nnU-Net provides strong baseline performance, and the MONAI framework provides healthcare-specific implementations. Commercial AI segmentation tools have emerged with FDA clearance for specific clinical use cases.
AI MRI segmentation supports clinical workflows in three main ways. First, quantitative measurement automation calculates tumor volumes, brain atrophy rates, cardiac ejection fractions, and liver fat fractions without manual measurement. Second, treatment response monitoring tracks changes in segmented regions across longitudinal imaging studies using standardized criteria like RECIST, mRECIST, RANO, PI-RADS, or LI-RADS. Third, surgical and treatment planning provides precise anatomical maps for neurosurgery, cardiothoracic surgery, hepatic resection, radiation therapy, and orthopedic procedures. Most FDA-cleared AI segmentation tools function as decision support, with radiologist verification of final findings.
The outlook for MRI segmentation with AI
MRI segmentation has progressed from manual outlining by trained anatomists to AI-augmented pipelines that produce segmentation maps in seconds rather than hours. The shift represents more than a speed improvement; it changes which clinical questions are tractable, which research populations are studyable, and which workflows are operationally viable at scale.
The direction of MRI segmentation through the next several years is multimodal, multi-organ, and clinically integrated. AI models trained on increasingly diverse datasets handle brain, cardiac, liver, and tumor segmentation through unified architectures rather than separate organ-specific models. Integration with PACS workflows lets segmentation outputs reach the radiologist’s reading workstation alongside the original imaging. Clinical decision support tools build on segmentation outputs to surface quantitative measurements that radiologists previously calculated manually. Multimodal segmentation that combines MRI with CT, ultrasound, and digital pathology data further extends the diagnostic scope.
For organizations evaluating AI-augmented imaging platforms, the segmentation capability is one component of a broader cloud-native imaging architecture. Vendor-neutral archives provide the storage layer into which segmentation outputs and DICOM imaging flow. Browser-based diagnostic viewers display segmentation results to clinicians without requiring specialized workstations. AI orchestration at the workflow level routes studies to appropriate segmentation models based on the clinical question. See Medicai’s overview of AI in radiology and cloud PACS platforms for the integration context within which AI segmentation operates.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo