Radiology Second Opinion: When to Get One, How It Works, Cost, and Turnaround

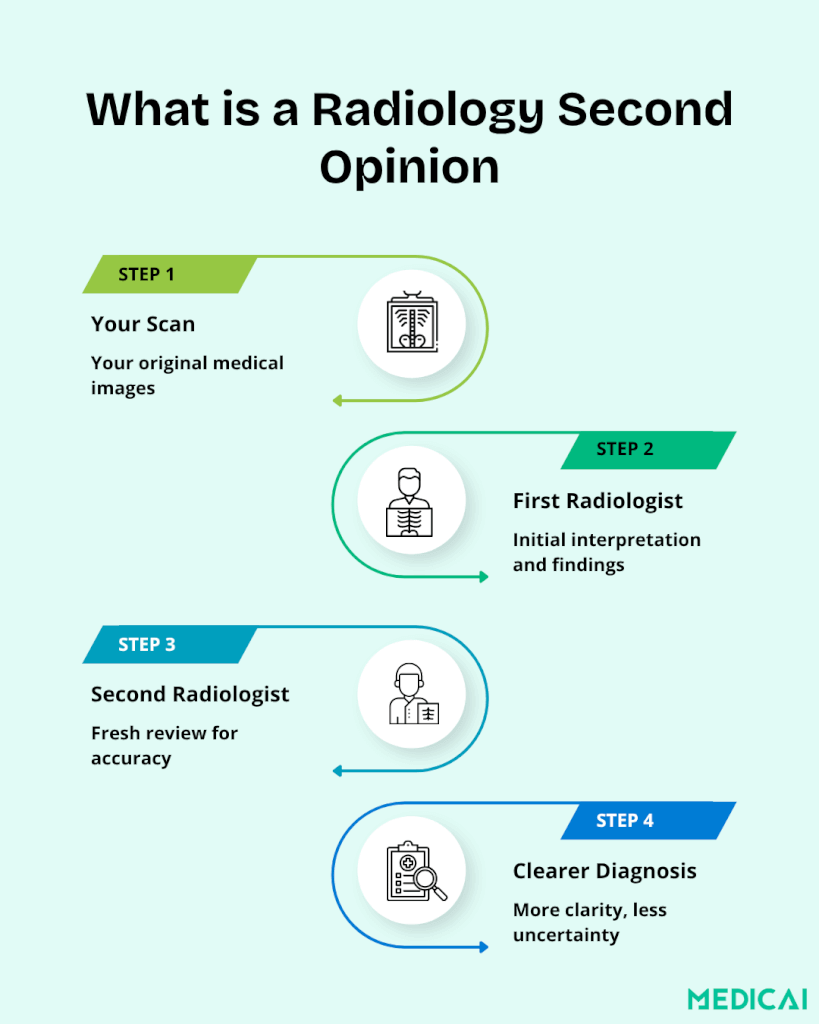
A radiology second opinion is an independent interpretation of an imaging study (MRI, CT, X-ray, ultrasound, mammography, PET, or other modality) by a radiologist other than the one who produced the original report. The second radiologist reviews the original images, generates an independent interpretation, and produces a second report that the patient and treating clinician can compare with the first. The clinical purpose is to confirm or revise diagnoses, particularly in cases involving cancer, complex pathology, ambiguous findings, or treatment decisions where the imaging interpretation directly drives the clinical decision.
The published research on the impact of second opinions is consistent: independent reinterpretation of imaging studies changes the diagnosis in a meaningful fraction of cases. Research from the Mayo Clinic shows that in 88% of cases, the diagnosis was refined or completely changed after a second review, demonstrating the clinical value of independent re-interpretation. Major academic medical centers (Mass General, Johns Hopkins, Mayo Clinic, Cleveland Clinic, UCLA, Penn Medicine, MD Anderson) operate dedicated second opinion radiology programs, and a growing market of dedicated commercial services (MDView, DocPanel, Verify Imaging, MedConsOnline) provides direct-to-patient and direct-to-provider access.
This guide covers the complete picture from the patient and treating clinician perspective: when to consider a second opinion, how the process works step by step, what to expect for turnaround time and cost, who provides the service, what the image transmission infrastructure requires, and how to interpret the second report against the first. For healthcare organizations deploying second opinion infrastructure at scale rather than seeking a single second opinion as a patient, see how medical image sharing works and the Medicai Medical Imaging Exchange.

What a Radiology Second Opinion Actually Means
A radiology second opinion involves another qualified radiologist reviewing your existing medical images, like MRI, CT scans, or X-rays. It provides an independent interpretation without any new tests or additional radiation. This second opinion offers a fresh perspective and helps minimize that uncertainty.
Research from the Mayo Clinic shows just how valuable a second opinion can be. In 88% of cases, the diagnosis was refined or completely changed after a second review. This proves that second opinions play a major role in improving accuracy and guiding patients toward the safest, most effective treatment plan.
Radiologists analyze patterns and details in scans, blending science and experience. As a result, two radiologists may focus on different aspects based on their backgrounds.
This is where sub-specialty expertise becomes important.
A general radiologist reads many types of scans every day. But a sub-specialist spends years reading the same type of scan over and over.
- A neuroradiologist looks at the brain and spine all day.
- A breast radiologist can detect subtle changes on mammograms and breast MRIs.
- A musculoskeletal (MSK) radiologist focuses on bones, joints, and sports injuries.
- A cardiac radiologist reads heart and vascular scans with a different lens.
Sub-specialists have unique training and expertise, allowing them to identify details that general radiologists might overlook or interpret differently. It can refine the diagnosis, confirm it, or point you toward a safer or more effective treatment path.
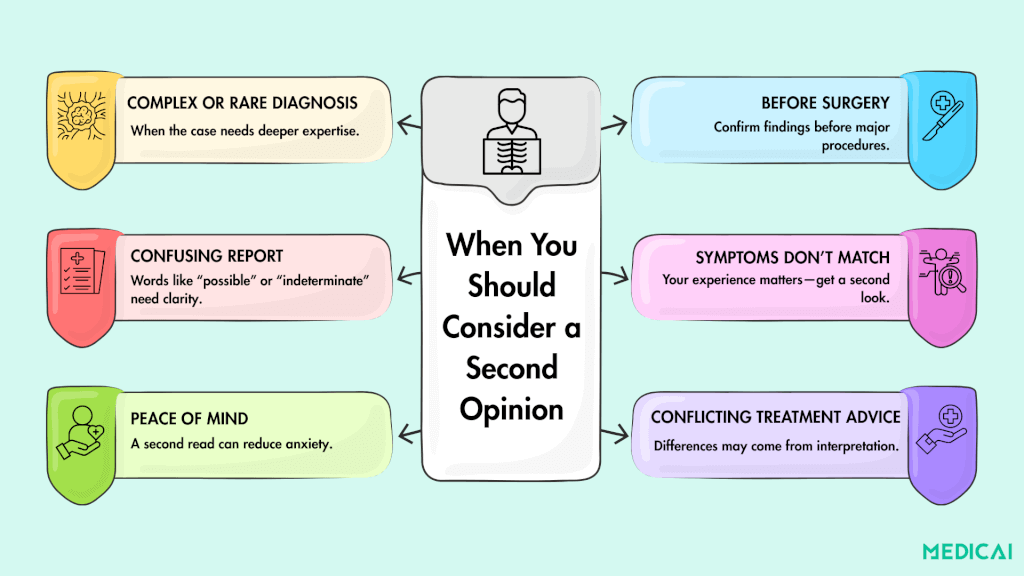
When You Should Consider a Radiology Second Opinion
Cancer Diagnosis and Staging
Cancer is the single most common reason patients seek a second radiology opinion. The imaging interpretation directly affects staging, treatment planning, and prognostic conversations. Specific scenarios where second-opinion radiology adds the most clinical value include initial cancer diagnosis when imaging findings are equivocal, staging studies that determine surgical candidacy or systemic treatment choice, restaging after initial treatment to assess response, and surveillance imaging when the question of recurrence hinges on subtle imaging change. Subspecialty review (a breast radiologist reading a breast MRI, a neuroradiologist reading a brain MRI, a pediatric radiologist reading a pediatric study) often produces a meaningfully different interpretation than a general radiology review of the same images.
Treatment Response Assessment
For cancer patients on systemic therapy, immunotherapy, or radiation, follow-up imaging assesses treatment response and guides next-step decisions. Treatment response criteria (RECIST, iRECIST, PERCIST for PET, Choi for sarcomas) involve specific measurement and classification rules that subspecialty radiologists apply more consistently than general radiology. Second-opinion review of treatment-response studies is common in oncology practice, particularly when the response category determines whether the patient continues the current treatment, switches treatments, or proceeds to surgery.
Not every scan needs a second opinion. But certain situations and scans may need a second opinion, as accuracy can affect treatment.
When the Diagnosis Is Complex or Rare
Some conditions are tricky. Tumors, neurological disorders, unusual joint injuries, or unexplained pain often need a deeper look. In these cases, small details can change the whole diagnosis.
A sub-specialty radiologist, someone who reads that exact type of scan every day, may spot patterns that others might overlook.
Before Major Surgery
If a surgery depends on imaging, you want to be absolutely sure the scan was read correctly.
Spine surgeries, joint replacements, tumor removals, or heart procedures often rely on tiny details on the MRI or CT. A second opinion can confirm the problem, clarify the severity, or even adjust the surgical plan.
In some cases, it may help you avoid surgery altogether.
When Imaging Results Are Confusing or Vague
Reports sometimes include phrases like “possible,” “likely,” “indeterminate,” or “cannot rule out.” These words are common in radiology, but they can leave patients unsure.
A second opinion helps turn vague language into a clearer answer. Another specialist may read the images through a different lens and provide you with more precise guidance.
When Your Symptoms Don’t Match the Report
If the report says “normal,” but you are still in pain, something doesn’t add up.
Radiology is powerful, but it isn’t perfect. Sometimes a finding is missed. Sometimes it looks different in context.
When your body tells you one thing, and the report tells you another, a second opinion can bring clarity.
When You Want Peace of Mind
Peace of mind is a valid medical reason. Even when the diagnosis is simple, some patients feel more secure with a second read, especially when dealing with cancer scares, chronic pain, or long-term conditions.
Knowing that two experts agreed can reduce stress and help you move forward with confidence.
When Treatment Decisions Conflict
Sometimes one doctor recommends surgery, while another suggests physical therapy.
Or one specialist sees “mild changes” while another sees “moderate.”
These differences usually come from how the scan was interpreted. Getting a second radiology read can help clarify the confusion and give you clearer direction.
Why Radiology Reads Can Differ: The Real Reasons Behind Interpretation Gaps
It can feel surprising when two radiologists give slightly different opinions on the same scan. But in reality, this happens more often than most people think.
- Imaging relies on human interpretation. Radiologists analyze patterns and subtle details, so different experts may focus on different findings.
- Training shapes perspective. Backgrounds in trauma, oncology, pediatrics, or general practice influence what each radiologist is trained to notice.
- Experience levels matter. Specialists who read the same type of scan daily develop stronger pattern recognition and may catch subtler issues.
- Sub-specialties see things differently. Neuroradiologists spot brain and spine nuances. MSK radiologists catch joint and ligament problems. Breast and cardiac specialists identify highly specific early changes.
- Image quality varies. Older machines or lower-resolution scans can hide important details.
- Context influences interpretation. Differences in clinical notes, history, or symptoms can lead to different but valid conclusions.
How the Radiology Second Opinion Process Works
The patient-facing process for obtaining a radiology second opinion follows the same general workflow across providers, with variation in cost, turnaround time, and submission method. The steps below describe the typical path.
Step 1: Obtain Your Original Imaging Study
The first step is to obtain your original imaging study in a format that the second-opinion radiologist can read. The clinically meaningful format is DICOM, the international standard for medical imaging data, which preserves the full image quality, slice information, and acquisition metadata that the radiologist needs for diagnostic interpretation. Most US hospitals and imaging centers provide DICOM imaging on CD-ROM or DVD when the patient requests it, typically at no charge or for a small administrative fee. The federal 21st Century Cures Act information blocking provisions strengthen patients’ right to access their own imaging in electronic form, and most facilities now also provide imaging downloads through online patient portals. What to avoid: JPEG images, screen captures, or printed films. These formats compress or transform the original DICOM data, thereby losing information that the radiologist needs for accurate interpretation.
Step 2: Choose a Second Opinion Provider
The choice of a second-opinion provider depends on the clinical question, the desired turnaround time, and the cost. Academic medical centers offer the deepest subspecialty expertise but typically operate on longer timelines and require a formal referral or direct contact with the center’s second-opinion program. Commercial second opinion services offer faster turnaround (often 24 to 72 hours) at published fee structures, with subspecialty matching for common clinical contexts. The landscape of named providers in the section below covers both categories.
Step 3: Submit the Imaging Study Securely
Once you have selected a provider, the imaging study is submitted to them. Modern second-opinion providers accept submissions through secure online platforms that handle DICOM transmission, HIPAA-compliant patient information handling, and chain-of-custody documentation. The submission typically includes the DICOM imaging study, the original radiology report (so the second radiologist can see what was previously concluded), relevant clinical history, and the specific clinical question driving the second-opinion request. Modern second-opinion providers operate a cloud-based image-transmission infrastructure that handles full-fidelity DICOM transfers with audit logging, encryption, and Business Associate Agreement coverage.
Step 4: The Second Opinion Radiologist Reviews
The second-opinion radiologist receives the imaging study via their reading workstation, opens it in their DICOM viewer, and reviews the images independently. Best practice for second opinion reading is to perform an initial review without first reading the original report (to avoid anchoring bias from the previous interpretation), then compare the independent reading against the original report once formed. Subspecialty second-opinion programs route the study to a radiologist with specialized expertise in the relevant anatomy or disease (e.g., breast imaging, neuroradiology, musculoskeletal imaging, body imaging, pediatric radiology, cardiac imaging, nuclear medicine).
Step 5: The Second Report Is Delivered
The second-opinion radiologist produces a structured report that includes the independent interpretation, a comparison of how the two reports differ, recommendations for additional imaging or clinical workup where appropriate, and the radiologist’s signature and credentials. The report is delivered to the patient and (with patient consent) to the treating clinician. Most second opinion services deliver the report through their secure online platform with PDF download for the patient and HL7 or secure email transmission to the treating physician’s office.
Step 6: Discuss the Second Report with Your Treating Clinician
The second opinion report is most useful when the patient and treating clinician discuss it together against the original report. The clinical decision-maker remains the treating physician, who integrates the imaging interpretation with the clinical context, examination findings, lab results, and patient preferences. When the two reports agree, the agreement reinforces confidence in the diagnosis. When they disagree, the disagreement opens specific questions: which interpretation better fits the clinical picture, whether additional imaging or biopsy is warranted to resolve the disagreement, and how the treatment plan should be adjusted given the new information.
What to Expect – Turnaround Time, Format, and Cost
The practical parameters of a second opinion (how long it takes, what the report looks like, how much it costs) vary significantly across providers. Understanding the range helps set realistic expectations and choose the right provider for the specific clinical situation.
Turnaround Time
Commercial second opinion services typically deliver reports in 24 to 72 hours from receipt of the imaging study, with expedited options available for urgent cases. Academic medical centers often operate on longer timelines (5 to 15 business days), reflecting deeper subspecialty review processes and tumor board or multidisciplinary discussions before finalizing the report. For cancer staging or treatment planning, where the next clinical decision depends on a second opinion, a faster commercial turnaround is often the practical choice. For complex or rare disease cases where subspecialty depth matters more than speed, the academic center timeline is usually worth the wait.
Report Format
A complete second opinion radiology report typically includes the patient identifying information and clinical context, the imaging modality and acquisition parameters reviewed, an independent description of findings (the body of the report), an impression section summarising the diagnostic conclusion, a comparison statement addressing any differences with the original report, recommendations for further evaluation if indicated, and the interpreting radiologist’s name, credentials, and signature. Some providers also include annotated images highlighting specific findings, which is particularly useful for ambiguous or subtle findings that the patient or referring physician may want to see directly.
Cost
Commercial second-opinion services typically charge between $100 and $500 per study, depending on the modality’s complexity, the required subspecialty, and the turnaround time. MRI and CT studies cost more than X-rays due to the higher complexity of review; subspecialty reads (pediatric, neuro, breast) cost more than general radiology; expedited turnaround carries a premium. Academic medical center second opinion programs vary in cost structure: some operate on a self-pay basis at price points similar to commercial services; others bill insurance under the radiology professional fee; and others provide second-opinion review as part of the broader oncology or specialty consultation visit at the center. Insurance coverage for second-opinion radiology is inconsistent. Some plans cover second-opinion radiology as a standard medical service when the treating physician orders it; others treat it as a non-covered service that the patient pays out of pocket. Before initiating a paid second opinion, patients should check coverage specifically with their insurer and document the clinical justification supporting medical necessity.
Is a Free Second Opinion Really Free?
Genuinely free, no-strings-attached radiology second-opinion services are rare. Most ‘free’ offerings operate one of two business models. The first model is a front-end conversion offer: the center or service offers the second opinion at no charge as the front end of a treatment relationship, hoping the patient will pursue care at that center if the second opinion confirms the need for treatment. The second model is research-based: the second opinion is provided in conjunction with clinical trial enrolment or research participation. Both models can provide useful clinical value to the patient, but the patient should understand the relationship before accepting a free offer. For a strictly independent second opinion without downstream commitment to a specific center or trial, the paid commercial or academic center routes are usually the appropriate choice.
Who Provides Radiology Second Opinion Services?
The US radiology second opinion market has two primary categories: academic medical centers operating dedicated programs and commercial direct-to-consumer services. Each category has strengths and limitations.
Academic Medical Center Second Opinion Programs
Major academic medical centers operate dedicated second-opinion radiology programs that combine deep subspecialty expertise with the multidisciplinary integration they provide. The named programs below are representative of the category.
Massachusetts General Hospital Imaging operates a second-opinion service through its imaging department, providing subspecialty review across the full range of radiology subspecialties and integrating with the broader Massachusetts General specialty consultation infrastructure. Johns Hopkins Radiology operates a similar second opinion service through its radiology department, with strong patient recognition reflected in the 40 monthly searches for ‘Johns Hopkins radiology second opinion’ specifically. Mayo Clinic provides second-opinion radiology as part of its broader specialty consultation program. Cleveland Clinic operates a second opinion program with international patient access. MD Anderson Cancer Center provides cancer-specific second-opinion radiology as part of its oncology consultation program. UCSF, UCLA, Stanford, Penn Medicine, and Memorial Sloan Kettering operate similar programs, generally available to patients through formal application or referral.
Commercial Direct-to-Consumer Second Opinion Services
Commercial second-opinion services have grown significantly since 2015, offering direct-to-patient access without requiring a formal application to an academic medical center. The major players in this category include MDView, DocPanel, Verify Imaging (secondopinions.com), MedConsOnline, Aristra, and American Telephysicians.
MDView is the dominant traffic-capturing service in this category, ranking at the top of several primary second-opinion search queries and receiving over 550 organic visits per month. MDView offers MRI and CT second opinions with subspecialty matching, online submission, and rapid turnaround. DocPanel operates a similar direct-to-consumer model with a strong educational content presence covering questions about the second-opinion process. Verify Imaging (operating at secondopinions.com) provides multi-specialty second opinion radiology, including subspecialty reads. MedConsOnline and Aristra offer similar direct-to-consumer second-opinion services, with variations in turnaround time, pricing, and subspecialty coverage.
The choice between academic and commercial second opinion services depends on the clinical context. For complex cancer cases requiring multidisciplinary discussion, academic center programs typically offer deeper integration. For straightforward second-opinion reads where the question is whether the original radiologist interpreted the study correctly, commercial services offer faster turnaround at a lower cost. The patient and treating clinician should choose based on the specific clinical question, not on brand recognition alone.
The Image Sharing Infrastructure Behind Second Opinion Radiology
The entire second-opinion radiology workflow depends on one critical step: transmitting the original imaging study from the patient or the originating facility to the second-opinion radiologist. The quality of this step determines whether the second-opinion process runs smoothly or fails due to logistical issues. Three properties of the image sharing infrastructure matter most.
DICOM Fidelity Preservation
The second opinion read must be performed on the original DICOM imaging data with full preservation of slice information, window-level settings, acquisition metadata, and image series structure. Compressed or converted images (JPEG, PDF screen captures, printed films) lose the information the radiologist needs for accurate interpretation. Any infrastructure used for second opinion image transfer must preserve full DICOM fidelity end to end, from the originating facility’s PACS through the transfer mechanism to the second opinion radiologist’s reading workstation.
HIPAA Compliance and Chain of Custody
Imaging data is Protected Health Information under HIPAA. Transfer infrastructure must operate under appropriate HIPAA safeguards: signed Business Associate Agreements between the patient or facility and the transfer platform; AES-256 encryption of DICOM data at rest; TLS 1.2 or higher encryption in transit; role-based access controls that limit who can view the study; and complete audit logging of access events. Older transfer mechanisms (mailing CD-ROMs, faxing images, emailing files) often fail to meet one or more of these requirements, creating HIPAA exposure for both the patient and the receiving radiologist.
Speed and Reliability
For urgent clinical situations (cancer staging before surgery, treatment response assessment, driving next-step decisions), the second opinion turnaround time is dominated by the image transfer step rather than the interpretation step. Modern cloud-based transfer infrastructure delivers a 200 MB CT study to the second opinion radiologist in minutes; legacy CD-ROM transfer takes days to weeks, including shipping and import. The speed difference directly affects the patient’s clinical timeline.
Where Medicai Fits
The Medicai Medical Imaging Exchange is the infrastructure platform that healthcare organizations and second opinion services use to handle the image transfer step of the workflow. The platform provides DICOM transfer with full fidelity preservation, HIPAA-compliant encryption and audit logging, a zero-footprint browser-based DICOM viewer for the receiving radiologist, and contractual Business Associate Agreement coverage. Medicai is not a second opinion service itself; Medicai does not employ radiologists and does not provide reads. Medicai is the underlying infrastructure that makes second-opinion radiology workflows operationally possible at scale, particularly for healthcare organizations that operate their own second-opinion programs or services and need scalable image-transfer infrastructure.
For patients seeking a single second opinion through an existing commercial service, the second-opinion provider typically handles the image-transfer infrastructure as part of their service. For healthcare organizations building or expanding second-opinion radiology capabilities, the choice of underlying infrastructure is a procurement decision in its own right. For healthcare organizations building or expanding second-opinion radiology capabilities, the choice of underlying infrastructure is a procurement decision in its own right. See how medical image sharing works for the standards and architecture involved.
Frequently Asked Questions
A radiology second opinion is an independent interpretation of an imaging study (MRI, CT, X-ray, ultrasound, mammography, PET, or other modality) by a radiologist other than the one who produced the original report. The second radiologist reviews the original DICOM images, generates an independent interpretation, and produces a second report that the patient and treating clinician can compare with the first. The clinical purpose is to confirm or revise diagnoses, particularly in cases involving cancer, complex pathology, ambiguous findings, or treatment decisions where the imaging interpretation directly drives the clinical decision. Research from the Mayo Clinic found that in 88% of cases, the diagnosis was refined or completely changed after a second review. Major academic medical centers (Mass General, Johns Hopkins, Mayo Clinic, Cleveland Clinic, MD Anderson) operate dedicated second-opinion programs, and commercial services, including MDView, DocPanel, Verify Imaging, and MedConsOnline, provide direct-to-patient second-opinion access.
The process has six steps. First, obtain your original MRI study in DICOM format from the imaging facility where it was performed, either on CD-ROM or through the facility’s online patient portal. The federal 21st Century Cures Act information blocking provisions strengthen your right to access your own imaging in electronic form. Second, choose a second opinion provider, either an academic medical center program or a commercial service, based on your clinical question, desired turnaround, and budget. Third, submit the DICOM imaging study to the provider through their secure online submission system, along with your original radiology report and relevant clinical history. Fourth, the second-opinion radiologist reviews the imaging study independently, typically with subspecialty matching to the relevant anatomy or disease. Fifth, the second opinion provider delivers a written report to you and (with your consent) to your treating physician. Sixth, discuss the second report with your treating clinician against the original report to determine the next clinical steps.
Commercial second opinion services typically charge between $100 and $500 per imaging study. The specific price depends on modality complexity (MRI and CT cost more than X-ray), subspecialty requirements (pediatric, neuro, and breast subspecialty reads cost more than general radiology), and turnaround time (expedited turnaround carries a premium). Academic medical center programs vary significantly in cost structure: some operate on a self-pay basis at price points similar to commercial services, others bill insurance under the radiology professional fee, and others bundle second-opinion review into broader specialty consultation visits. Insurance coverage for second-opinion radiology is inconsistent. Some plans cover it as a standard medical service when ordered by the treating physician, while others treat it as a non-covered service paid out of pocket. Before initiating a paid second opinion, patients should check coverage with their insurer and document the clinical justification (e.g., confirmation of cancer diagnosis, surgical planning, treatment response assessment) that supports medical necessity.
Genuinely free, no-strings-attached radiology second-opinion services are rare. Most “free” offerings operate one of two business models. The first model is a front-end conversion offer: the center or service offers the second opinion at no charge as the front end of a treatment relationship, hoping the patient will pursue care at that center if the second opinion confirms the need for treatment. The second model is research-based: the second opinion is provided in conjunction with clinical trial enrolment or research participation. Both models can provide useful clinical value to the patient, but the patient should understand the downstream implications before accepting a free offering. For a strictly independent second opinion without commitment to a specific center or trial, the paid commercial or academic center routes are usually the appropriate choice. Some patient advocacy organizations and cancer-specific foundations also sponsor free second opinions for patients with specific diagnoses, which is a legitimate third path worth exploring for cancer patients in particular.
Commercial second opinion services typically deliver reports within 24 to 72 hours of receipt of the imaging study, with expedited options available for urgent cases at a premium. Academic medical center programs typically operate on longer timelines, ranging from 5 to 15 business days, reflecting deeper subspecialty review and multidisciplinary discussion processes. The total elapsed time from initiating the request to receiving the report includes three components: the image transfer step (which can take days if using CD-ROM or other legacy mechanisms, or minutes if using modern cloud-based transfer infrastructure), the interpretation step (24 hours to 15 business days depending on provider), and the report delivery step (typically same-day once interpretation is complete). For urgent clinical situations where the next decision depends on a second opinion, commercial services with cloud-based transfer infrastructure typically yield the fastest overall timeline. For complex cases where subspecialty depth matters more than speed, academic center timelines are usually worth the wait.
The clinical answer is: obtain your imaging study in DICOM format from the originating facility (request a CD-ROM or download it through the patient portal), then submit the DICOM study to the second-opinion provider through their secure online submission system. Most modern second-opinion providers operate cloud-based DICOM submission platforms that handle transfers with full image fidelity, HIPAA-compliant encryption, audit logging, and contractual Business Associate Agreement coverage. Avoid sending compressed images (JPEG, PDF, screen captures) because these lose information the radiologist needs for accurate interpretation. If your provider does not have an online submission portal, secure file sharing through HIPAA-compliant services is the next-best option; email is not appropriate for unencrypted PHI transfer. For healthcare organizations operating their own second-opinion programs or services that handle many image transfers per month, the choice of underlying infrastructure (a cloud-based image-sharing platform with full DICOM fidelity preservation) is a procurement decision in its own right. The Medicai Medical Imaging Exchange (link: medicai.io/products/medical-imaging-exchange) is one example of the infrastructure platform that powers image transfer for second opinion workflows at an organizational scale.
Conclusion
A radiology second opinion is a specific clinical tool with a specific clinical role. The strongest cases for seeking one are cancer diagnosis and staging, treatment response assessment, surgical planning, complex multi-system disease, ambiguous findings on the original report, and disagreement between imaging and clinical findings. Commercial services deliver second opinions within 24 to 72 hours for $100 to $500 per study; academic medical center programs offer deeper subspecialty integration over longer timelines. The image transfer step matters as much as the interpretation step for the overall workflow to succeed. For individual patients seeking a single second opinion, the existing commercial services and academic programs handle the workflow end-to-end. For healthcare organizations building second opinion capability at scale, the underlying infrastructure (cloud PACS with DICOM image sharing) is a procurement decision in its own right.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo