RIS-PACS Integration: HL7 Messaging, DICOM Modality Worklist, and Failure Prevention

For a Radiology IT Director, there is no headache quite like “Interface Fatigue.”
You have a Radiology Information System (RIS) handling the scheduling and billing. You have a PACS handling the images. And sitting between RIS PACS integration is a fragile web of HL7 interfaces that dictates whether your workflow runs smoothly or grinds to a halt.
RIS-PACS integration does not operate in isolation — it sits within a three-layer stack. The EHR (Electronic Health Record) or EMR generates the imaging order and receives the completed report. The RIS manages the radiology-specific workflow between the order and the report. The PACS stores and serves the images produced during the exam. HL7 messages connect all three layers: HL7 ORM carries the order from EHR to RIS, the RIS MWL extends it to the modality, and HL7 ORU returns the result from PACS through RIS back to the EHR.
When these systems fall out of sync, the consequences are immediate: broken links, lost orders, and the dreaded “typo” that creates a phantom patient record.
This guide is not a glossary of terms; it is a technical breakdown of how to maintain data integrity between your administrative and clinical layers, and why modern practices are moving toward Brokerless Integration and HL7 FHIR messaging.

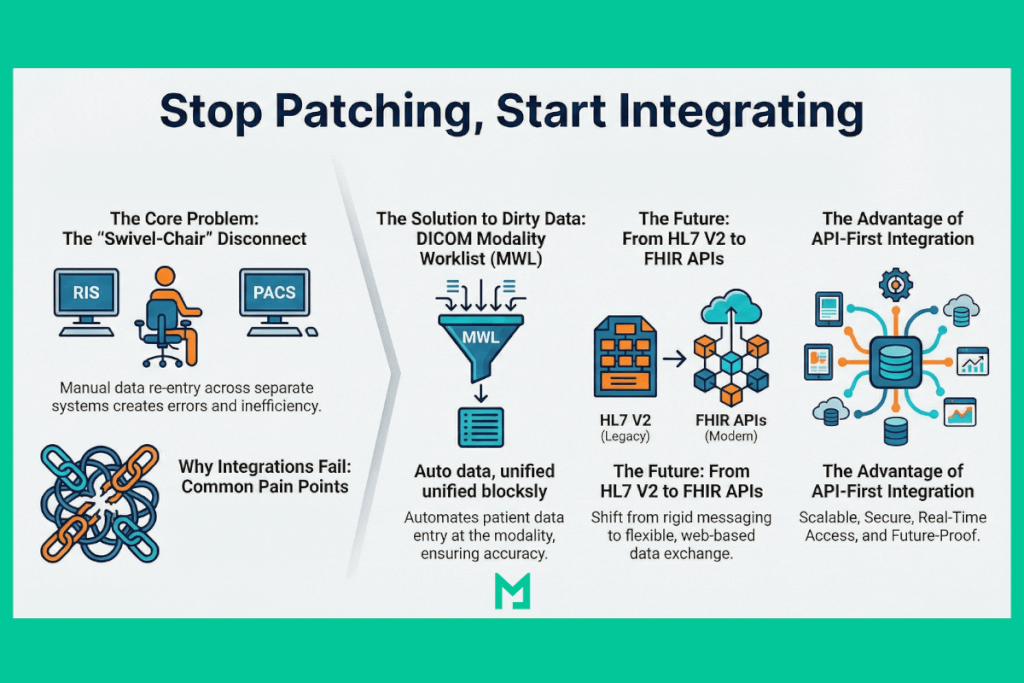
The Core Problem: The “Swivel-Chair” Disconnect
In a legacy environment, the RIS and PACS systems are separate data silos with some significant differences. Without tight integration, a technologist might manually type patient demographics into the modality console.
This introduces human error. A typo in the Patient ID or a missing Accession Number breaks the link between the image and the order. The radiologist opens the PACS system to read the study, but the images aren’t thereâthey are floating in the “Unassigned” folder because the metadata didn’t match.
To prevent this, we rely on a specific synchronization language. Here is a summary of the core problems and solutions through RIS PACS integration.
The Language of Synchronization: HL7 ORM and ORU
The backbone of RIS-PACS integration relies on HL7 V2 messages. Understanding the flow of these messages is critical for troubleshooting “lost” studies.
HL7 ORM (Order Entry)
Direction: RIS to PACS/Modality
When a patient is scheduled in the RIS, the system generates an HL7 ORM message. This message pushes the Patient Demographics (Name, DOB, MRN) and the specific Accession Number (the unique ID for that particular exam) to the PACS and the Modality Worklist.
- The Risk: If the PACS doesn’t receive the ORM, it doesn’t know the patient is coming.
HL7 ORU (Observation Result)
Direction: PACS/Voice Recognition to RIS
Once the radiologist dictates the report, the PACS sends an HL7 ORU message back to the RIS. This updates the status from “Examined” to “Finalized” and triggers the billing process.
- The Risk: If the ORU fails, the report remains “stuck” in the PACS, the referring doctor never gets the result, and the claim is never billed.
DICOM Modality Worklist (MWL): How It Eliminates Data Entry Errors in RIS-PACS Integration
DICOM Modality Worklist (MWL) is a DICOM service that allows an imaging modality — CT scanner, MRI, X-ray unit — to query a server (typically the RIS) for the list of scheduled examinations it should process, pulling patient demographics and accession numbers directly rather than relying on manual technologist entry.
To eliminate manual data entry errors, you must implement a strict DICOM Modality Worklist (MWL).
Instead of the technologist typing “John Smith” into the CT scanner, the scanner queries the RIS Worklist server. It pulls down the exact demographics and Accession Number generated by the HL7 ORM message.
This ensures that the DICOM tags attached to the images match the RIS record character-for-character. When the images arrive at the PACS, they auto-reconcile with the order. No manual intervention required.

Why Integrations Fail: Common Pain Points
Even with MWL, data integrity issues persist. Here are the common failure points we see in legacy architectures:
- Unidirectional Sync: Many older interfaces only push data one way. If a receptionist corrects a patient’s name in the RIS after the order is sent, the PACS is never updated, creating a split record.
- Split Accession Numbers: If a patient has a Chest X-ray and a Rib X-ray ordered separately but scanned together, legacy systems often struggle to merge the images into a single view.
The “Interface Engine” Tax — and Why It Fails Silently
Traditional RIS-PACS environments route every HL7 message through a third-party interface engine — Mirth Connect, Cloverleaf, Rhapsody, or similar middleware — that translates messages between vendor-specific implementations. On paper, this solves the interoperability problem. In practice, it creates a maintenance burden and a category of failure that is uniquely dangerous in clinical environments: the silent failure.
What silent failure mean in an interface engine context
When an HL7 interface engine fails, the failure is not always visible to clinical staff. The engine may continue accepting inbound messages and returning positive acknowledgement (ACK) responses to the sending system, which tells the RIS “message delivered successfully,” while the downstream PACS never receives the message. From the RIS’s perspective, the order was sent. From the PACS’s perspective, the patient does not exist. From the technologist’s perspective, the worklist is empty, and they enter demographics manually. From the radiologist’s perspective, the images are present but lack a matching order and sit in the unassigned queue. No alert fires. No system generates an error. The failure propagates silently until a clinician calls to ask why results are missing.
This happens because most HL7 V2 implementations treat the ACK as a transport confirmation rather than a processing confirmation. The interface engine acknowledges receipt of the message at the network level, but whether the translated message is successfully written to the downstream system is a separate transaction that may fail independently—and often does, particularly after software upgrades on either end of the interface.
The three most common silent failure scenarios
- The first is the post-upgrade interface break. When either the RIS or PACS vendor releases a software update, the message structure may change in ways that break the interface engine’s translation rules — a field may move, a delimiter may change, or a new required segment may be added. The interface engine continues routing messages, but the receiving system rejects them silently at the application layer. This is the most common cause of a sudden drop in worklist population that appears unrelated to any system event, because the upgrade on one system was completed days earlier, and the interface failure is discovered only when the throughput drops.
- The second is the unidirectional sync gap. Most legacy interface engines are configured to push messages in one direction at the time of the original order — RIS to PACS when the study is scheduled. If a patient’s demographics are corrected in the RIS after the order has been sent — a misspelled name, a corrected date of birth, a merged duplicate MRN — the correction generates a new HL7 ADT (Admit, Discharge, Transfer) message that must be separately configured to route to the PACS. In many installations, this ADT route was never set up. The PACS retains the original incorrect demographics indefinitely, creating a split record that affects every study acquired under the wrong identity.
- The third is the accession number collision. When the RIS generates an accession number that collides with an existing entry in the PACS — due to differences in numbering formats between systems, counter resets after system migrations, or prefix changes between departments — the PACS either silently rejects the incoming study or incorrectly merges it with a prior study. The technologist acquires the study, it transmits to PACS successfully at the DICOM level, and then disappears from the worklist because the accession number lookup finds a conflict and drops the study into an exception queue that is monitored by no one.
The maintenance cost that accumulates invisibly
Beyond silent failures, interface engines impose an ongoing maintenance cost that is rarely budgeted correctly at implementation time. Every software upgrade on the RIS, the PACS, or the interface engine itself requires retesting every configured interface — verify that ORM messages still route correctly, that ORU responses return on sign-off, that ADT updates propagate, that MWL queries still resolve. In a department running three modalities connected to two RIS instances and one PACS, that is potentially a dozen interface paths to retest after every upgrade cycle. The testing is manual, time-consuming, and performed under pressure because upgrades are typically scheduled during maintenance windows when clinical operations cannot be disrupted for long.
This is the “interface engine tax” in its full form: not just licensing cost (Mirth Connect, Cloverleaf, and Rhapsody carry annual licensing in the range of $15,000–$80,000 depending on message volume and deployment model), but the accumulated cost of an IT engineer’s time spent maintaining, testing, and debugging a layer of infrastructure that exists solely to compensate for the lack of a native integration standard between systems. The move toward FHIR-native integration eliminates this layer by replacing point-to-point message translation with a standardised API that both systems speak natively — no translation engine, no ACK ambiguity, no post-upgrade regression testing of interface paths.
The Future: From HL7 V2 to FHIR APIs
The industry is reaching the limits of what HL7 V2 can handle. It is brittle, chatty, and requires heavy maintenance.
Modern architectures, like Medicai, are moving toward bi-directional synchronization using HL7 FHIR vs. V2 standards.
The Advantage of API-First Integration
Instead of waiting for a “push” message (V2), a FHIR-enabled system can “pull” data in real-time via web APIs.
- True Interoperability: Your PACS doesn’t just store images; it serves as a Vendor Neutral Archive (VNA), normalizing data from different RIS providers without complex interface engines.
- Instant Demographics Updates: If a patient record is updated in the EHR/RIS, the API reflects that change in the PACS archive immediately.
- Hybrid Speed: By combining cloud scalability with Hybrid PACS architecture, you can ensure that even heavy 3D datasets are available instantly, with metadata perfectly synced across the enterprise.
| Capability | HL7 V2 interface engine | HL7 FHIR API |
|---|---|---|
| Data update model | Push only — the sending system initiates every message; the receiving system cannot request data on demand | Bidirectional — either system can push updates or pull current data via RESTful API calls at any time |
| Patient demographics sync | Batch at order time — demographics are sent once when the order is created; corrections require a separately configured ADT message route that is often missing in legacy deployments | Real-time — any update to the patient record in the EHR or RIS is immediately available to the PACS via the Patient resource endpoint; no separate ADT route required |
| Failure detection | Silent ACK — the interface engine returns a positive acknowledgement at the transport layer even when the downstream system has not processed the message; failures are discovered hours later when results are missing | Observable HTTP response — every API call returns a standard HTTP status code (200, 400, 404, 500); failures are immediately visible to the calling system and can trigger automated alerts |
| Post-upgrade maintenance | Manual retesting required after every software upgrade on either end — message structure changes can break translation rules silently; each interface path must be verified individually | Versioned API contracts — the FHIR specification versions the API independently of application upgrades; breaking changes are managed through versioned endpoints rather than ad-hoc message structure changes |
| Infrastructure overhead | Requires a dedicated interface engine server (Mirth Connect, Cloverleaf, Rhapsody) with licensing costs of $15,000–$80,000 annually plus an IT engineer to maintain translation rules and monitor message queues | No middleware layer — both systems communicate directly via HTTPS; infrastructure overhead is limited to API key management and endpoint configuration |
| EHR-PACS image access | Report text delivered to EHR via HL7 ORU; images require a separate PACS viewer login — clinician navigates two systems to see both report and images | SMART on FHIR launch — the EHR can launch a zero-footprint DICOM viewer in context directly from the patient record, surfacing images and report in a single interface without a separate login |
FAQ: RIS-PACS Integration
What is RIS-PACS integration?
RIS-PACS integration is the technical connection between a Radiology Information System and a Picture Archiving and Communication System that enables the two systems to exchange patient data, exam orders, and report information automatically, without manual data entry at any point in the workflow. The integration operates across two protocol layers: HL7 V2 messaging handles the administrative data flow — imaging orders travel from EHR to RIS as HL7 ORM messages, and completed radiology reports return from PACS to RIS as HL7 ORU messages — while the DICOM Modality Worklist handles the clinical data flow, delivering scheduled exam demographics from the RIS directly to the imaging modality so the technologist does not need to type patient information manually before acquisition. When both layers are functioning correctly, a patient registered at the front desk automatically appears on the radiology worklist with accurate demographics, the acquired images arrive in PACS correctly tagged to the matching order, and the signed report reaches the referring physician’s EHR without any manual step in between.
How does PACS work with RIS?
PACS and RIS work together through a specific sequence of message exchanges tied to each stage of the imaging exam. When a clinician orders an imaging exam in the EHR, an HL7 ORM message flows to the RIS, which registers the order and assigns an accession number. The RIS then writes the scheduled exam data — patient name, MRN, date of birth, accession number, exam description — to the DICOM Modality Worklist server. The imaging modality queries the worklist using DICOM C-FIND before acquisition, pulling the exact demographics into its console. After acquisition, the modality sends the completed DICOM study to PACS using C-STORE. The PACS matches the incoming study to the open RIS order using the accession number as the linking key. When the radiologist signs the report, the PACS generates an HL7 ORU message that travels back to the RIS, updating the study status from “Examined” to “Finalized” and triggering billing. The RIS then distributes the report to the referring physician’s EHR via a second HL7 ORU message. Every hand-off in this sequence depends on the accession number remaining consistent across all systems — when it does not, studies detach from their orders and require manual reconciliation.
Is RIS a component of PACS?
No. RIS and PACS are architecturally separate systems built on different standards and designed for different functions. PACS manages imaging data — DICOM files, image storage, retrieval, and the diagnostic viewing tools radiologists use to interpret studies. RIS manages administrative data — patient scheduling, exam ordering, technologist worklists, report distribution, and billing. They are connected by HL7 interfaces and the DICOM Modality Worklist, but neither system contains or depends on the other’s software. In some enterprise radiology platforms — particularly cloud-native systems — RIS and PACS functionality is delivered through a unified interface that makes the two systems appear as one, but even in these deployments, the underlying data models remain distinct: text-based administrative records governed by HL7 standards on one side, pixel-based imaging data governed by DICOM standards on the other. Describing RIS as a component of PACS is like describing the front desk as part of the operating theatre — both are necessary for the same patient journey, but they are different rooms running different processes.
How does HIS fit into RIS-PACS integration?
A Hospital Information System (HIS) is the enterprise layer that sits above both RIS and PACS in the integrated radiology stack. HIS manages the master patient index — the authoritative record of patient identity across the entire hospital — along with admissions, discharge, transfer, and insurance data. In the imaging workflow, data flows downward from HIS: when a patient is admitted, the HIS generates an HL7 ADT (Admit, Discharge, Transfer) message that creates or updates the patient record in the RIS. When a physician orders an imaging exam, the HIS generates the HL7 ORM order that initiates the RIS scheduling workflow. The RIS then handles everything downstream — worklist, acquisition, reporting, billing — and sends results back upward via HL7 ORU to HIS and EHR. The practical implication is that patient identity errors originating in HIS — a misspelled name, an incorrect date of birth, a duplicate MRN — propagate downward through RIS into PACS and into the DICOM headers of every study acquired for that patient. Fixing a patient identity error in HIS does not automatically correct it in RIS or PACS without bidirectional ADT message routing configured at each interface layer.
What is the difference between HL7 V2 and FHIR for PACS integration?
HL7 V2 and FHIR (Fast Healthcare Interoperability Resources) are both standards for exchanging healthcare data, but they operate on fundamentally different architectures with different implications for PACS integration. HL7 V2 is a message-based standard: systems push pipe-delimited text messages to each other at predefined trigger events — order created, study completed, report signed. Each message must be translated by an interface engine if the sending and receiving systems use different vendor implementations. The interface engine adds infrastructure costs, maintenance overhead, and a silent-failure risk: messages are lost without generating an alert. FHIR is an API-based standard: systems expose RESTful endpoints that any authorised client can query or update in real time using standard HTTP. A FHIR-enabled PACS can pull the current patient demographics from the EHR at any time rather than waiting for a push message, detect failed API calls immediately via HTTP status codes rather than discovering lost messages hours later, and surface DICOM images directly within the EHR interface using SMART on FHIR launch — allowing a clinician to open the imaging study from the patient’s EHR record without a separate PACS login. The migration from HL7 V2 to FHIR is the defining infrastructure shift in modern RIS-PACS integration, eliminating the interface engine middleware layer and replacing per-upgrade interface regression testing with versioned API contracts.
Stop Patching, Start Integrating
If your IT team spends more time fixing broken links than optimizing workflows, it is time to look at your architecture.
Legacy “interface patches” are a temporary fix for a structural problem. By adopting a cloud-native, API-first imaging strategy, you can move beyond simple message passing and achieve true Brokerless Integration.
For radiology practices evaluating the financial impact of integration reliability, the connection between PACS data quality and billing outcomes is covered in detail in the radiology revenue cycle management guide.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo