Orthopedic Imaging: Modalities, Clinical Use Cases, and Surgical Workflow

Orthopedic imaging is the application of medical imaging to the diagnosis, surgical planning, and postoperative assessment of musculoskeletal conditions, including bone fractures, joint disorders, soft-tissue injuries, spinal conditions, and degenerative changes. The clinical scope spans five primary imaging modalities (plain-film X-ray, magnetic resonance imaging, computed tomography, ultrasound, and dual-energy X-ray absorptiometry, or DEXA), each addressing different anatomic structures and clinical questions. A typical orthopedic patient encounter involves at least one imaging study, and complex cases such as joint replacement, complex fracture management, and spinal surgery routinely involve multiple modalities acquired across the diagnostic, pre-operative, and post-operative phases of care.
The clinical purpose of orthopedic imaging differs from that of general radiology in two specific ways. First, the imaging is task-directed: the orthopedic surgeon typically already knows the anatomic region of interest and the suspected pathology, and the imaging confirms or refines that working diagnosis rather than discovering it. Second, the imaging is workflow-integrated: orthopedic imaging is often the input to surgical planning, digital templating, and intra-operative reference, which means the imaging acquisition, interpretation, and storage must operate within a workflow that supports those downstream uses. The imaging infrastructure side of this workflow (the orthopedic PACS, templating tools, and pre-operative planning capabilities) is covered in detail in the Medicai orthopedic PACS and templating guide.
This guide covers the clinical inputs side of orthopedic imaging: the five primary imaging modalities used in orthopedic practice; the clinical use cases by body region and subspecialty; the workflow from imaging acquisition through interpretation to surgical planning; and the comparison of modalities for common orthopedic indications. It is written for orthopedic practice administrators, imaging operations leaders, and clinicians evaluating their imaging service line or PACS infrastructure, and assumes general familiarity with the clinical practice of orthopedic surgery and sports medicine.
Imaging Modalities Used in Orthopedics: Five Primary and Two Adjunct
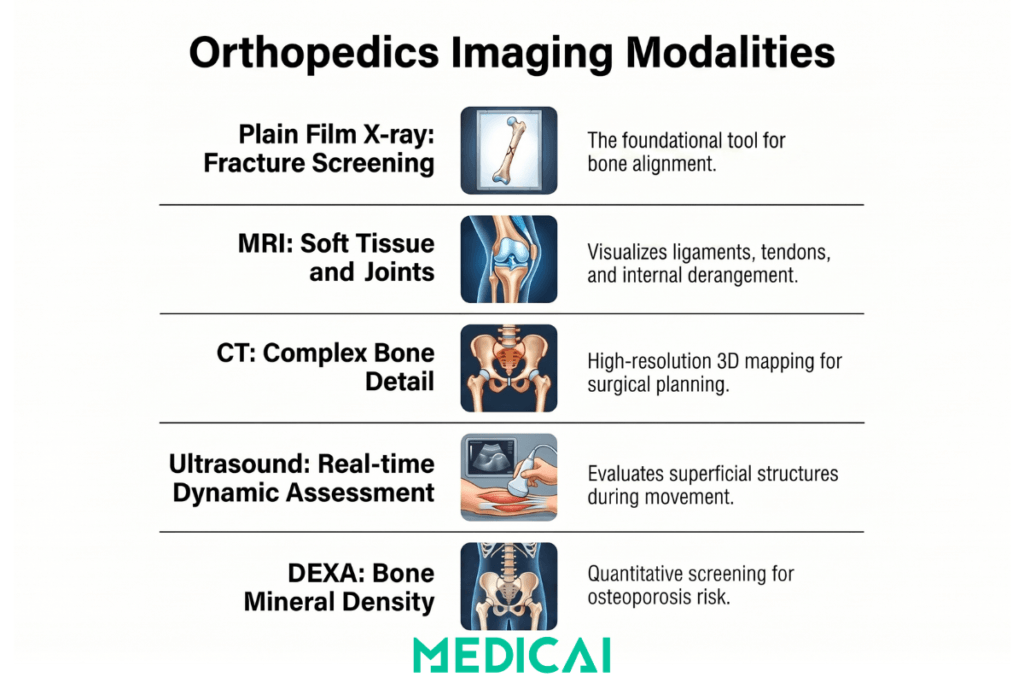
Orthopedic imaging draws on five primary imaging modalities and two adjunct modalities used in specific subspecialty contexts. The choice of modality for a given clinical question is governed by the American College of Radiology (ACR) Appropriateness Criteria and the American Academy of Orthopedic Surgeons clinical practice guidelines, both of which provide indication-specific guidance for modality selection.
1. Plain Film X-ray (Radiography)
Plain film X-ray remains the foundational orthopedic imaging modality and the most commonly performed orthopedic imaging study by a wide margin. It is the primary screening modality for fracture detection, joint alignment assessment, post-operative implant evaluation, and skeletal survey. The modality is fast (typically two to three minutes of imaging time), inexpensive relative to MRI and CT, widely available across hospitals, urgent care centers, and outpatient orthopedic clinics, and produces images that orthopedic surgeons interpret routinely without requiring formal radiology consultation for most straightforward findings.
The clinical applications of plain-film X-ray in orthopedics include initial fracture diagnosis and characterization, alignment assessment for joint replacement planning, weight-bearing views for lower-extremity alignment, scoliosis assessment in spinal radiography, post-operative implant position verification, and surveillance imaging for healing assessment. Standard projections (anteroposterior, lateral, oblique) are tailored to the specific anatomic region being imaged, with specialised views (sunrise, mortise, scaphoid, sunrise, axillary) added for specific clinical questions. The limitations are real: plain film does not visualize soft-tissue structures, including cartilage, ligaments, tendons, and menisci, and subtle or nondisplaced fractures may not appear on initial radiographs.
2. Magnetic Resonance Imaging (MRI)
Orthopedic MRI is the modality of choice for assessing soft tissues and internal joint structures. Where plain film visualizes bone, MRI visualizes everything else: cartilage, ligaments, tendons, menisci, labrum, muscles, neurovascular structures, and the bone marrow itself. Orthopedic MRI is the standard for evaluating internal derangement of the knee (meniscus tears, anterior and posterior cruciate ligament injuries, articular cartilage assessment), rotator cuff and labral pathology in the shoulder, hip labral tears, and femoroacetabular impingement, spine assessment for disc herniation and spinal stenosis, and most sports medicine soft tissue injuries.
The clinical workflow for orthopedic MRI typically follows initial plain-film imaging when soft-tissue pathology is suspected, the clinical examination suggests internal derangement, or pre-operative planning requires detailed visualization of structures that plain-film imaging cannot demonstrate. Field strength and imaging protocols matter clinically: 3 Tesla scanners produce higher resolution images than 1.5 Tesla scanners, and dedicated extremity coils improve image quality for hand, wrist, foot, and ankle imaging. Contrast administration (gadolinium) is used in specific contexts, including postoperative imaging to distinguish scar tissue and recurrent pathology, evaluation of suspected infection, and tumor characterization. The cost is substantial (typical US charges for orthopedic MRI range from $1,000 to $4,000 per study), and access varies: urgent and same-day MRI is routinely available in tertiary centers but may involve multi-day waits in some community settings.
3. Computed Tomography (CT)
Orthopedic CT provides high-resolution bone detail and is the modality of choice for complex fracture characterization, pre-operative surgical planning of bony procedures, three-dimensional reconstruction for deformity assessment and surgical planning, and evaluation of bone pathology that requires more detail than plain film can provide. CT is faster than MRI (with typical acquisition times under two minutes), more widely available than MRI in emergency settings, and produces images that can be reformatted into multiplanar reconstructions and three-dimensional renderings for surgical planning.
Specific clinical applications include complex articular fractures (tibial plateau, calcaneus, acetabulum, distal radius) where surgical planning requires understanding the three-dimensional fracture geometry, pre-operative templating for complex revision joint replacement, spine surgical planning where bony detail is critical (pedicle screw placement, deformity correction, fusion assessment), and assessment of bone tumors and metastases. The radiation dose from orthopedic CT is significant (a pelvic CT delivers approximately 6 millisieverts, equivalent to two years of background radiation exposure), which limits its routine use, particularly in pediatric and younger adult populations, where cumulative radiation exposure matters more.
4. Musculoskeletal Ultrasound
Musculoskeletal ultrasound has grown substantially as an orthopedic imaging modality over the past decade, driven by improvements in transducer technology, the availability of office-based ultrasound in orthopedic and sports medicine practices, and the modality’s specific advantages for real-time dynamic assessment and image-guided procedures. Ultrasound visualizes superficial soft-tissue structures, including tendons, ligaments, muscles, peripheral nerves, joint effusions, and bursae, with excellent resolution, and its real-time imaging capability supports dynamic assessment that static MRI cannot provide.
Specific orthopedic ultrasound applications include rotator cuff assessment, Achilles and other tendon evaluation, lateral epicondylitis and other tendinopathies, peripheral nerve evaluation, including carpal tunnel and ulnar nerve assessment, joint effusion characterization, and image-guided injections (corticosteroid injections for joint pathology, platelet-rich plasma injections for tendinopathy, hyaluronic acid injections for osteoarthritis). The advantages over MRI include real-time imaging that allows dynamic assessment of structures under load, point-of-care imaging that can be performed during the office visit, lower cost (typical US charges range from $200 to $800), and absence of contraindications related to implanted devices or claustrophobia. The limitations include operator dependence (image quality depends heavily on the sonographer’s skill and experience), limited visualization of deeper structures and bone interiors, and field-of-view constraints that make whole-joint assessment more difficult than with MRI.
5. Dual-Energy X-ray Absorptiometry (DEXA / DXA) for Bone Densitometry
DEXA scanning measures bone mineral density and is the standard imaging modality for osteoporosis screening and monitoring. The clinical purpose differs from the other four modalities: DEXA does not visualize anatomic structures for fracture or pathology diagnosis; instead, it produces quantitative measurements (T-score and Z-score) that classify the patient’s bone density relative to a young adult reference population and an age-matched reference population. The World Health Organization criteria define osteoporosis as a T-score of -2.5 or lower, and osteopenia as a T-score between -1.0 and -2.5.
The clinical applications of DEXA in orthopedic practice include osteoporosis screening in patients at risk for fragility fractures (postmenopausal women, men over 70, patients with risk factors including chronic corticosteroid use), monitoring of osteoporosis treatment response over time, fracture risk assessment integrated with clinical risk factors using tools like FRAX, and pre-operative bone density assessment before joint replacement or spinal fusion where implant fixation depends on bone quality. The radiation dose is very low (less than one-tenth the dose of a chest X-ray), and the typical study takes 15 to 20 minutes, including patient positioning.
Adjunct Modalities: Fluoroscopy and Nuclear Medicine
Fluoroscopy provides real-time X-ray imaging during procedures and is used in orthopedic practice for intraoperative guidance of fracture reduction, implant placement, vertebroplasty and kyphoplasty, image-guided injections, and joint arthrography. The C-arm fluoroscopy unit is standard equipment in orthopedic operating rooms and is also used in interventional pain management and image-guided procedures performed in office or procedure room settings.
Nuclear medicine imaging, including bone scintigraphy and PET-CT, has more focused indications in orthopedic practice. Bone scan imaging detects increased bone turnover associated with stress fractures, occult fractures, infection, and metastatic disease, and is particularly useful when plain films are negative but clinical suspicion remains high. PET-CT has growing applications in orthopedic oncology for staging and assessing treatment response in primary bone tumors and soft tissue sarcomas.
Clinical Use Cases by Body Region and Subspecialty
Orthopedic imaging organizes around the body region being imaged and the orthopedic subspecialty managing the patient. The modality selection, imaging protocols, and clinical workflow differ across these contexts. The sections below cover the most common orthopedic imaging contexts.
Sports Medicine Imaging
Sports medicine imaging addresses musculoskeletal injuries sustained in athletic activity, ranging from acute traumatic injuries (ligament tears, fractures, dislocations) to chronic overuse injuries (tendinopathies, stress fractures, joint cartilage degeneration). The clinical reality of sports medicine imaging is that patients are typically younger than the general orthopedic population, recovery and return-to-play decisions depend on accurate imaging interpretation, and time to imaging matters because delayed diagnosis can delay treatment and prolong return to activity.
The imaging workflow in sports medicine typically begins with plain-film X-ray to rule out fracture or significant bony pathology, followed by MRI when soft-tissue injury is suspected, and clinical examination findings warrant further evaluation. Ultrasound has grown as a point-of-care modality for sports medicine practices, supporting real-time dynamic assessment, in-office diagnosis of tendon and ligament pathology, and image-guided therapeutic injections. Common sports medicine imaging contexts include ACL and other knee ligament evaluation, rotator cuff and shoulder labral pathology, ankle ligament injuries, stress fracture evaluation in runners and other endurance athletes, and tendinopathy assessment.
Joint Replacement and Arthroplasty Imaging
Joint replacement imaging spans the pre-operative, intra-operative, and post-operative phases of total hip, total knee, and shoulder arthroplasty procedures. Pre-operative imaging includes weight-bearing plain-film X-rays for component sizing and alignment planning, CT for complex revision cases or when significant deformity is present, and MRI in selected cases where soft-tissue pathology affects surgical planning. The digital templating workflow that translates this imaging into the surgical plan is covered in the Medicai Orthopedics PACS and Templating Guide.
Post-operative imaging includes immediate post-operative plain films for implant position verification, surveillance imaging at standard intervals to monitor implant alignment and the bone-implant interface, and targeted imaging when the patient presents with post-operative pain, instability, or suspected complications. The imaging workflow integration matters here as much as the imaging itself: pre-operative imaging must be accessible for surgical reference, post-operative imaging must be available for comparison with pre-operative status, and longitudinal imaging series must be retained for monitoring throughout the typical 10 to 20-year implant lifespan.
Spine Imaging
Spine imaging spans cervical, thoracic, lumbar, and sacral evaluation for degenerative disease, disc pathology, deformity (scoliosis, kyphosis), trauma, infection, tumor, and post-operative assessment. Plain film X-ray remains the initial modality for trauma evaluation, alignment assessment, and post-operative imaging. MRI is the modality of choice for disc and neural element evaluation, supporting diagnosis of disc herniation, spinal stenosis, nerve root compression, and other neural causes of pain. CT is used to assess bony detail, particularly in pre-operative planning for spinal fusion and deformity correction, where pedicle anatomy and bone quality influence screw placement and construct selection.
The clinical workflow for spine imaging typically combines plain film and MRI for initial diagnostic evaluation, with CT added for pre-operative planning when surgery is indicated. Specialized studies, including flexion-extension plain films, CT myelography (when MRI is contraindicated), and dynamic MRI, add value in specific clinical scenarios. Spine surgery practices accumulate substantial imaging volumes per patient, given the sequential evaluation across multiple modalities and the longitudinal follow-up imaging across the course of care.
Hand, Wrist, and Upper Extremity
Hand, wrist, and upper extremity imaging emphasizes high-resolution evaluation of small anatomic structures, including the small bones of the wrist, the digital tendons and pulleys, the intrinsic ligaments of the wrist, and the peripheral nerves passing through the carpal tunnel and Guyon’s canal. Plain film is the initial modality for fracture evaluation, with specialized views (scaphoid view, oblique views, ulnar deviation views) used to demonstrate specific anatomic regions. Dedicated extremity MRI scanners and small extremity coils on standard MRI produce high-resolution images that visualize small ligaments and tendons that whole-body imaging cannot resolve.
Musculoskeletal ultrasound has grown particularly in this body region, given the superficial location of most clinically relevant structures and the value of dynamic assessment. Common hand and wrist ultrasound applications include evaluation of carpal tunnel syndrome (median nerve assessment), de Quervain’s tenosynovitis, trigger finger evaluation, and image-guided injections for tendon sheath pathology.
Foot and Ankle
Foot and ankle imaging combines weight-bearing plain-film evaluation (essential for alignment and biomechanical assessment), MRI for soft-tissue and internal joint pathology, CT for complex fractures and surgical planning, and ultrasound for tendon and ligament evaluation, including the Achilles tendon, peroneal tendons, and plantar fascia. Stress fractures are a common diagnostic challenge in this body region, with plain film often negative in the early stages and MRI or bone scan needed to confirm the diagnosis when clinical suspicion is high.
Paediatric Orthopedics
Pediatric orthopedic imaging applies the same modalities to a population where radiation exposure considerations are more weighty, where growing skeletons present imaging findings (growth plates, ossification centers) that adult imaging does not include, and where age-specific orthopedic conditions, including developmental dysplasia of the hip, slipped capital femoral epiphysis, Legg-Calve-Perthes disease, and idiopathic scoliosis, affect the imaging approach. Plain film remains the foundation, with ultrasound playing a substantial role in pediatric hip evaluation (including developmental dysplasia screening in infants) and in other contexts where radiation exposure is to be avoided. MRI is increasingly used in pediatric orthopedics for the same reason: it avoids radiation in a population where cumulative dose over a long lifetime matters.
The Orthopedic Imaging Workflow
The orthopedic imaging workflow extends from clinical encounter through imaging acquisition, interpretation, surgical planning, and post-operative follow-up. The workflow stages below describe the typical sequence; specific orthopedic practices and subspecialty contexts may vary from this pattern.
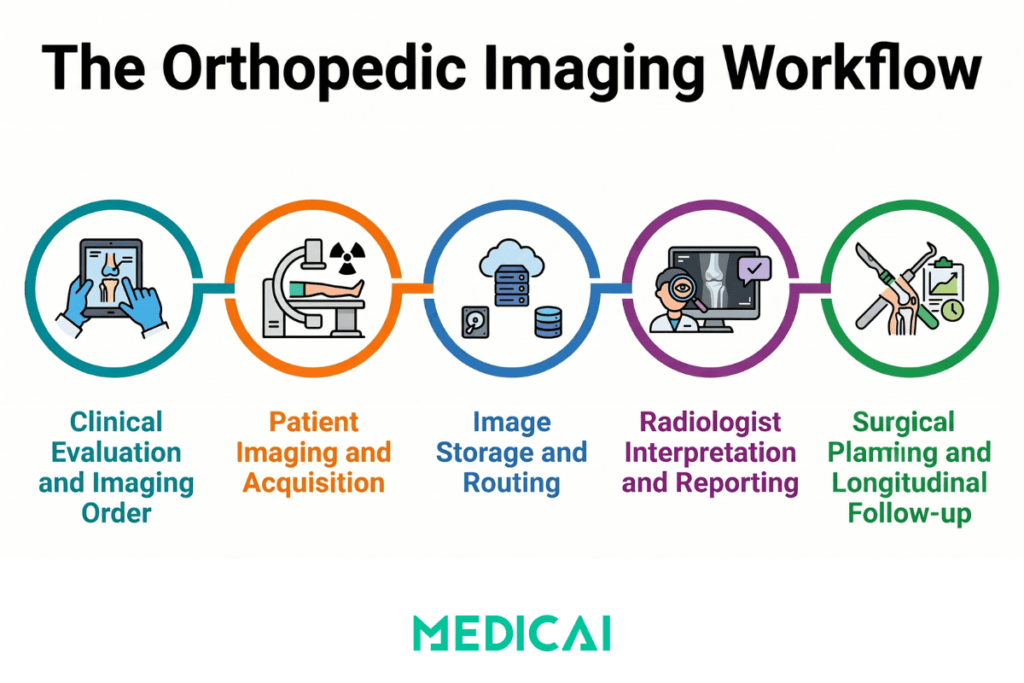
Stage 1: Clinical evaluation and imaging order.
The orthopedic encounter begins with history, physical examination, and clinical assessment that identify the suspected pathology, the anatomic region of interest, and the appropriate imaging modality. The imaging order specifies the body part, the clinical indication, and the requested imaging protocol. Modern orthopedic practices use electronic ordering integrated with the EHR, with orders flowing to the imaging facility via HL7 ORM messages or through direct EHR integration when the imaging facility uses the same EHR system.
Stage 2: Imaging acquisition.
The patient is positioned and imaged at the imaging modality (X-ray room, MRI scanner, CT scanner, ultrasound suite). The technologist follows the acquisition protocol specific to the body part and clinical indication, producing the imaging series that the radiologist will interpret. Image quality at this stage depends on appropriate patient positioning, modality-specific technical factors (kVp and mAs for X-ray and CT, pulse sequences for MRI, transducer selection and frequency for ultrasound), and adherence to the acquisition protocol for the specific clinical question.
Stage 3: Image storage and worklist routing.
The acquired imaging study is transmitted via DICOM from the modality to the PACS, where it is stored, made available for radiologist interpretation through the reading worklist, and eventually delivered to the orthopedic practice for clinical use. The PACS infrastructure that handles this stage in orthopedic-specific deployments is covered in the Medicai orthopedic PACS and templating guide. Worklist routing may include subspecialty matching, so a sports medicine MRI is routed to a sports medicine radiologist at a practice with that subspecialty depth.
Stage 4: Radiologist interpretation.
The radiologist reviews the imaging study, applies the clinical context from the order, and produces a structured diagnostic report. Subspecialty musculoskeletal radiologists provide deeper interpretation for complex orthopedic cases, particularly in sports medicine, tumor imaging, and complex post-operative evaluation. The structured reporting workflow that produces the report is covered in the Medicai structured radiology reporting guide.
Stage 5: Surgical planning and templating.
For surgical orthopedic cases, the imaging supports digital templating and pre-operative planning. The orthopedic surgeon reviews the imaging in the PACS viewer, applies templating software to size and align components, saves the surgical plan, and references it during the procedure. This stage is the focal point of the sister orthopedic PACS and templating workflow.
Stage 6: Post-operative imaging and longitudinal comparison.
Post-operative imaging is compared with pre-operative imaging to confirm surgical execution, identify any post-operative complications, and monitor healing over time. The imaging archive must retain pre-operative, operative, and post-operative imaging in a way that supports easy comparison years after the original procedure, particularly for joint replacement surveillance, where implant lifespan spans decades.
PACS and Templating Infrastructure for Orthopedic Imaging
The imaging modalities and clinical workflow described above operate on top of a PACS infrastructure layer that handles the storage, retrieval, viewing, and surgical planning of orthopedic imaging studies. Orthopedic practices have specific PACS requirements beyond general radiology PACS, including digital templating capability for joint replacement planning, calibration tools for component sizing, multi-modality comparison for combined plain film and MRI evaluation, and integration with the surgical planning tools used pre-operatively and intra-operatively.
The Medicai cloud-native orthopedic PACS combines DICOM storage on Microsoft Azure infrastructure, a zero-footprint browser-based viewer with orthopedic-specific tools, integrated digital templating, and cross-site access supporting the desktop-to-OR continuity that orthopedic surgical workflows require. The full architecture, the templating workflow, and the operational benefits for practice managers and CIOs are covered in the sister Medicai orthopedic PACS and templating guide. For organizations evaluating orthopedic PACS procurement specifically, see the Medicai orthopedic PACS solution.
Orthopedic Imaging Modalities Compared at a Glance
| Modality | Primary clinical use | Strengths | Limitations | Typical cost (US) |
|---|---|---|---|---|
| Plain film X-ray (radiography) | Initial fracture detection, joint alignment, post-operative implant assessment, skeletal survey | Fast acquisition (2 to 3 minutes), widely available, low cost, immediate interpretation by orthopedic surgeons for most findings | No soft tissue visualisation; subtle fractures may not appear; two-dimensional projection of three-dimensional anatomy | $50 to $250 per study |
| MRI (magnetic resonance imaging) | Soft tissue and internal joint structure assessment: ligaments, tendons, cartilage, menisci, labrum, neural structures | Superior soft tissue contrast, no ionising radiation, multiplanar imaging, three-dimensional reconstruction | Higher cost than other modalities, longer acquisition time (30 to 60 minutes), limited availability in some settings, contraindications for some implanted devices and patient claustrophobia | $1,000 to $4,000 per study |
| CT (computed tomography) | Complex fracture characterisation, pre-operative bony surgical planning, three-dimensional reconstruction | High-resolution bone detail, fast acquisition (under 2 minutes), multiplanar reconstruction, three-dimensional rendering | Meaningful radiation dose (limits use in paediatric and younger adult populations), limited soft tissue contrast compared to MRI | $500 to $2,500 per study |
| Musculoskeletal ultrasound | Superficial soft tissue evaluation, dynamic assessment, image-guided injections, point-of-care imaging | Real-time dynamic imaging, point-of-care availability, no radiation, lower cost, no contraindications | Operator-dependent quality, limited deep structure visualisation, limited bone interior assessment, narrower field of view | $200 to $800 per study |
| DEXA (bone densitometry) | Osteoporosis screening, fracture risk assessment, monitoring of osteoporosis treatment response | Quantitative bone density measurement, very low radiation dose, standardised T-score and Z-score reporting | Does not visualise anatomic pathology; specific to bone density assessment rather than general orthopedic imaging | $100 to $300 per study |
Frequently Asked Questions
Orthopedic imaging is the application of medical imaging to the diagnosis, surgical planning, and postoperative assessment of musculoskeletal conditions, including bone fractures, joint disorders, soft-tissue injuries, spinal conditions, and degenerative changes. The clinical scope spans five primary imaging modalities: plain film X-ray for initial fracture detection and joint alignment, magnetic resonance imaging for soft tissue and internal joint structures, computed tomography for complex fracture characterization and pre-operative bony surgical planning, musculoskeletal ultrasound for superficial soft tissue and dynamic assessment, and dual-energy X-ray absorptiometry (DEXA) for osteoporosis screening and bone density measurement. Each modality addresses distinct anatomic structures and clinical questions, and the American College of Radiology Appropriateness Criteria and the American Academy of Orthopedic Surgeons clinical practice guidelines guide the choice of modality for a given clinical scenario.
The imaging modality depends on the suspected condition and the anatomic region. Plain film X-ray is typically the initial study for suspected fractures, joint alignment assessment, and most acute orthopedic complaints. MRI is the modality of choice for soft tissue injuries including ligament tears (ACL, rotator cuff), meniscus pathology, tendon injuries, and labral pathology. CT is used for complex fractures (tibial plateau, acetabulum, calcaneus, complex spine fractures) and pre-operative bony planning. Musculoskeletal ultrasound is used for superficial soft tissue evaluation, dynamic assessment of tendon function, and image-guided injections. DEXA is used specifically for bone density measurement in osteoporosis screening. Most orthopedic patients undergo at least one imaging study, and complex cases routinely involve multiple modalities sequenced across the diagnostic, pre-operative, and post-operative phases of care.
Typical US charges vary significantly by modality. Plain film X-ray ranges from approximately $50 to $250 per study and is the most affordable orthopedic imaging modality. CT scans range from approximately $500 to $2,500 per study depending on the body region and whether contrast is administered. MRI is the most expensive routine orthopedic imaging modality, with charges ranging from approximately $1,000 to $4,000 per study depending on body region, contrast administration, and facility. Musculoskeletal ultrasound ranges from approximately $200 to $800 per study and is often performed in office by sports medicine and orthopedic practices. DEXA scans for bone densitometry range from approximately $100 to $300 per study. Insurance coverage varies; diagnostic orthopedic imaging coverage is provided when ordered by a physician for medically indicated reasons; out-of-pocket costs depend on the insurance plan, deductible status, and whether the imaging is performed in-network.
The terms are largely synonymous in clinical practice but carry slightly different connotations. “Orthopedic imaging” is used more commonly in orthopedic surgery, sports medicine, and primary care contexts, where imaging supports orthopedic clinical decisions. “Musculoskeletal imaging” or “MSK imaging” is the term more commonly used in the radiology subspecialty context, referring to the subspecialty that focuses on interpreting musculoskeletal conditions. Subspecialty musculoskeletal radiologists complete dedicated fellowship training in interpreting orthopedic imaging across all modalities. The two terms describe overlapping content from different perspectives: orthopedic imaging from the clinical user perspective, musculoskeletal imaging from the radiology subspecialty perspective.
Sports injury imaging typically begins with plain-film X-ray to rule out fracture or significant bony pathology, followed by MRI when soft-tissue injury is suspected, and clinical examination findings warrant further evaluation. Common sports injury imaging contexts include ACL and other knee ligament evaluation (MRI is the standard), rotator cuff and shoulder labral pathology (MRI, often supplemented with ultrasound for dynamic assessment), ankle ligament injuries (plain film for fracture rule-out, MRI for soft tissue characterisation), stress fracture evaluation in runners and other endurance athletes (plain film often negative in early stages; MRI or bone scan needed when clinical suspicion is high), and tendinopathy assessment (ultrasound has grown as the point-of-care modality, MRI used for deeper or more complex pathology). Musculoskeletal ultrasound has grown particularly in sports medicine practice, given its real-time dynamic assessment capabilities and office-based point-of-care availability.
Orthopedic imaging integrates with PACS through standard DICOM protocols, with the imaging studies stored, retrieved, and viewed through the PACS infrastructure. Orthopedic-specific PACS adds capabilities beyond general radiology PACS, including digital templating for joint replacement planning, calibration tools for component sizing from plain-film images, multimodal comparison views for combined plain-film and MRI evaluation, and integration with preoperative surgical planning tools. The workflow extends from imaging acquisition through PACS storage, radiologist interpretation, surgeon review with templating, pre-operative plan finalization, intra-operative reference, and post-operative comparison with the pre-operative imaging. Modern cloud-native orthopedic PACS platforms support this workflow with desktop-to-OR continuity, allowing the surgeon to perform templating in the office, save the plan, and reference it on an iPad or wall monitor in the operating room. The full architecture and operational benefits are covered in the Medicai orthopedic PACS and templating guide; the procurement-level evaluation is covered in the Medicai orthopedic PACS solution.


Related Articles
Lets get in touch!
Learn more about how Medicai can help you strengthen your practice and improve your patients’ experience. Ready to start your Journey?
Book A Free Demo